Genetic Information
Gene & Transcript Details
| ID | Status | Details |
|---|---|---|
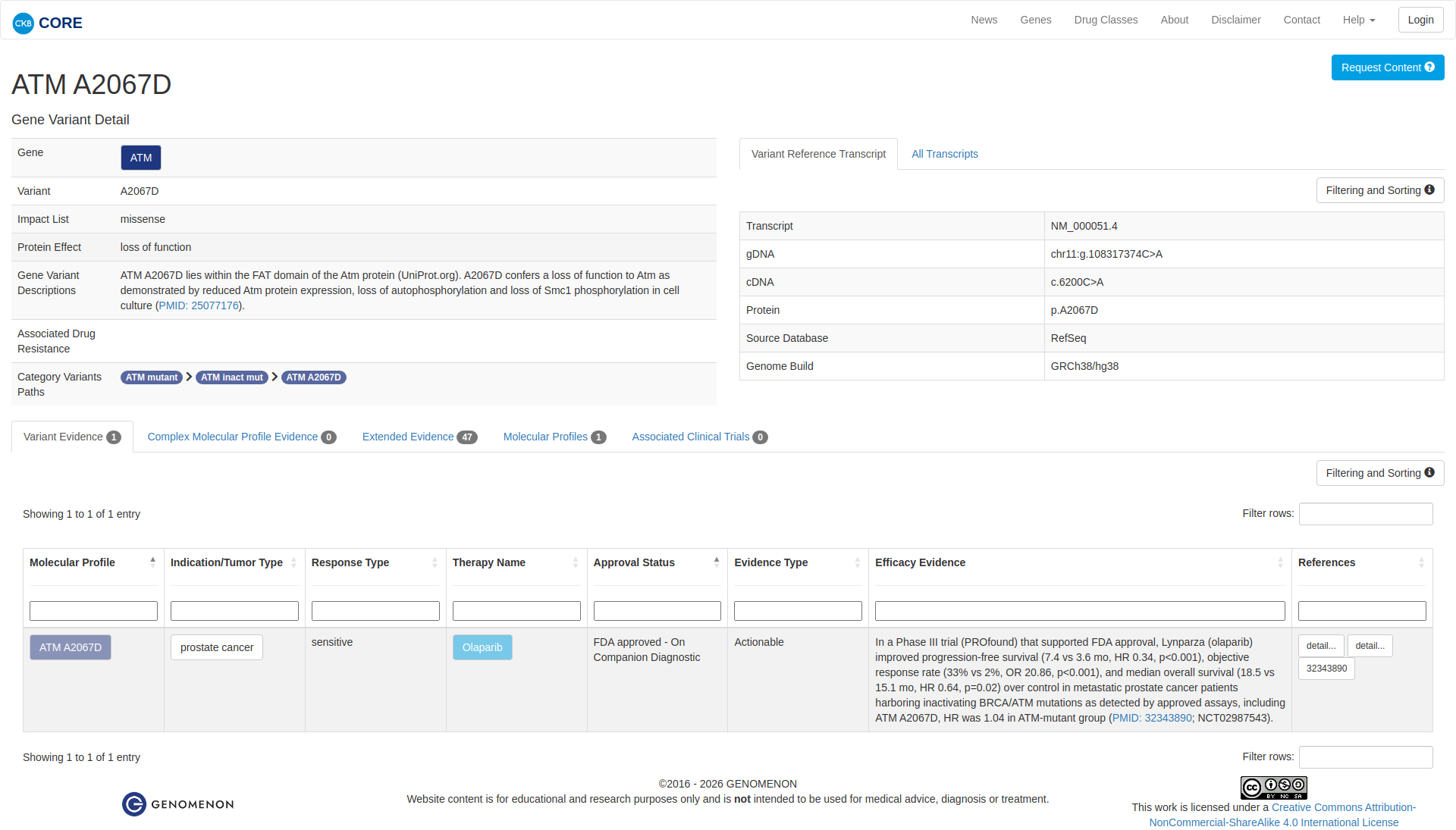
| NM_000051.3 | RefSeq Select | 13147 nt | 386–9556 |
| NM_000051.4 | MANE Select | 12915 nt | 151–9321 |
Variant Details
Clinical & Population Data
Population Frequency
gnomADClinVar
OpenThe p.A2067D pathogenic mutation (also known as c.6200C>A), located in coding exon 42 of the ATM gene, results from a C to A substitution at nucleotide position 6200. The alanine at codon 2067 is replaced by aspartic acid, an amino acid with dissimilar properties. This alteration has been reported in two individuals/families with ataxia-telangiectasia (Sandoval N et a. Hum. Mol. Genet. 1999 Jan; 8(1):69-79; Dawson AJ et al. Am. J. Med. Genet. 2015 Aug;167A(8):1937-9). This alteration has also been shown to segregate with primary-appearing dystonia in homozygous individuals from three Canadian Mennonite families (Saunders-Pullman R et al. Neurology. 2012 Feb; 78(9):649-57). Additionally, functional assays demonstrated that this alteration results in reduced protein expression, absent autophosphorylation, and diminished transphorphylation of downstream ATM targets (Nakamura K et al. Mol Genet Genomic Med. 2014 Jul; 2(4):332-40). Based on internal structural analysis, this variant is anticipated to result in a significant decrease in structural stability (Ambry internal data). This amino acid position is well conserved in available vertebrate species. This variant is considered to be rare based on population cohorts in the Genome Aggregation Database (gnomAD). In addition, the in silico prediction for this alteration is inconclusive. Based on available evidence to date, this variant is unlikely to be causative of classical ataxia-telangiectasia; however, it may be associated with dystonia and may lead to increased risk of developing ATM-related cancer. Based on the supporting evidence, this alteration is interpreted as a disease-causing mutation.
This sequence change replaces alanine, which is neutral and non-polar, with aspartic acid, which is acidic and polar, at codon 2067 of the ATM protein (p.Ala2067Asp). This variant is present in population databases (rs397514577, gnomAD 0.0009%). This missense change has been observed in individual(s) with ataxia-telangiectasia (A-T) (PMID: 9887333, 22345219, 25914063; internal data). It has also been observed to segregate with disease in related individuals. ClinVar contains an entry for this variant (Variation ID: 39749). An algorithm developed to predict the effect of missense changes on protein structure and function (PolyPhen-2) suggests that this variant is likely to be disruptive. Experimental studies have shown that this missense change affects ATM function (PMID: 25077176). For these reasons, this variant has been classified as Pathogenic.
The c.6200C>A variant in ATM is a missense variant predicted to cause substitution of alanine to aspartic acid at amino acid 2067. This variant is rare in the general population with a frequency below the threshold expected for the associated phenotype(s). This variant has been observed in one or more individuals affected with the associated recessive disease, as either homozygous or compound heterozygous with a second variant (PMID: 25077176). Given the available evidence, this variant is classified as Pathogenic.
This variant is considered likely pathogenic. This variant has been reported in multiple individuals with clinical features of gene-specific disease [PMID: 19650357, 22345219, 25077176]. Functional studies indicate this variant impacts protein function [PMID: 19650357, 25077176].
This missense variant replaces alanine with aspartic acid at codon 2067 of the ATM protein. Computational prediction suggests that this variant may not impact protein structure and function. This variant has been reported in multiple individuals affected with breast cancer (PMID: 20305132, 26898890; Color internal data) and pancreatic cancer (Color internal data). This variant has been reported in the homozygous or compound heterozygous state in individuals affected with typical or mild ataxia telangiectasia (PMID: 9887333, 22345219, 25037873, 25077176, 25914063). Lymphoblastoid cells isolated from homozygous carriers have shown absent to trace levels of ATM protein, reduced ATM kinase activity, and increased sensitivity to radiation, indicating reduced capacity to repair DNA damage (PMID: 22345219, 25077176). This variant has been identified in 1/251316 chromosomes in the general population by the Genome Aggregation Database (gnomAD). Based on the available evidence, this variant is classified as Pathogenic.
"This variant has been reported in ClinVar as Likely pathogenic (5 clinical laboratories) and as Pathogenic (11 clinical laboratories) and as pathogenic (1 clinical laboratories)."
COSMIC Somatic Evidence
Open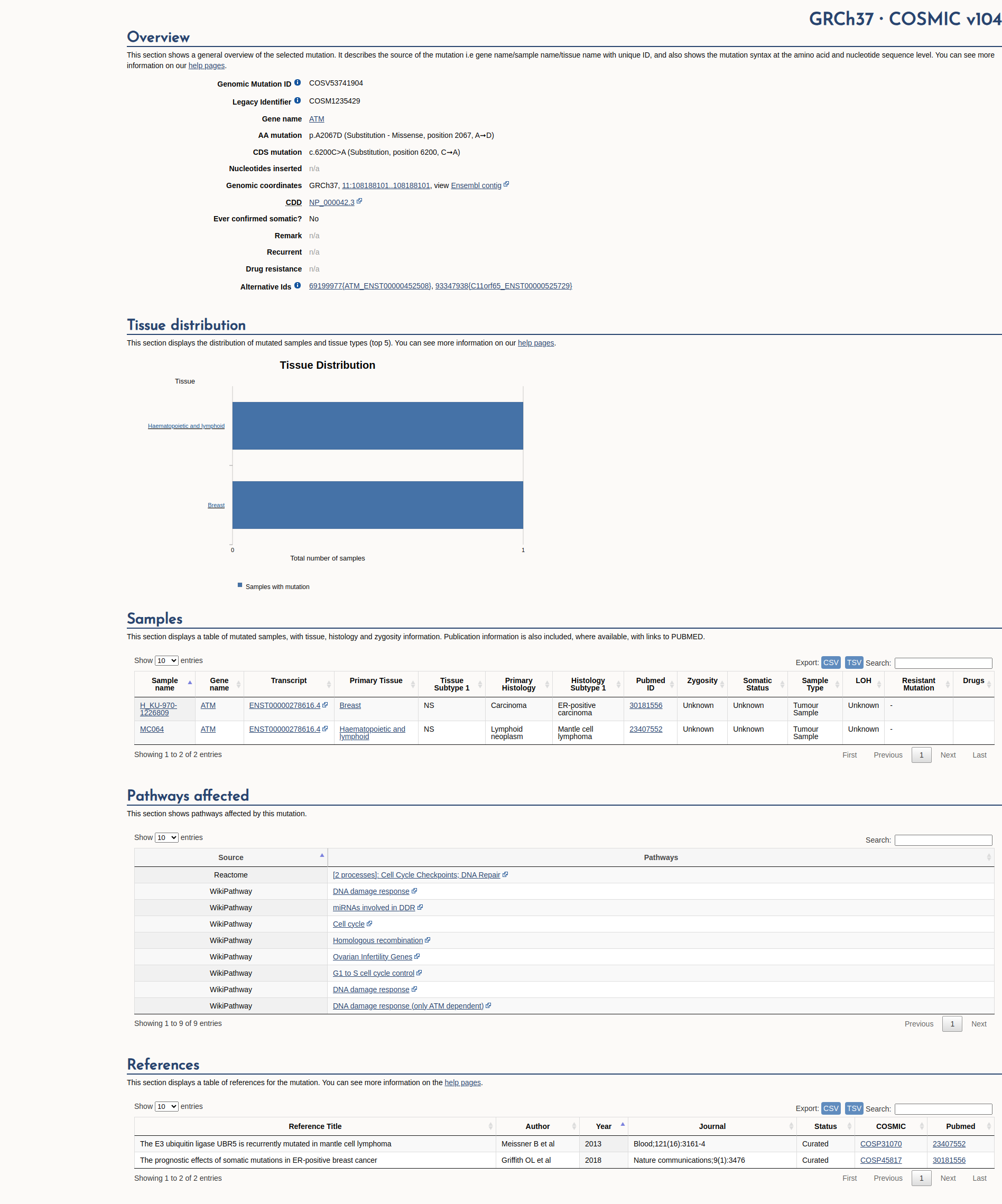
Functional Impact & Domains
Functional Domain
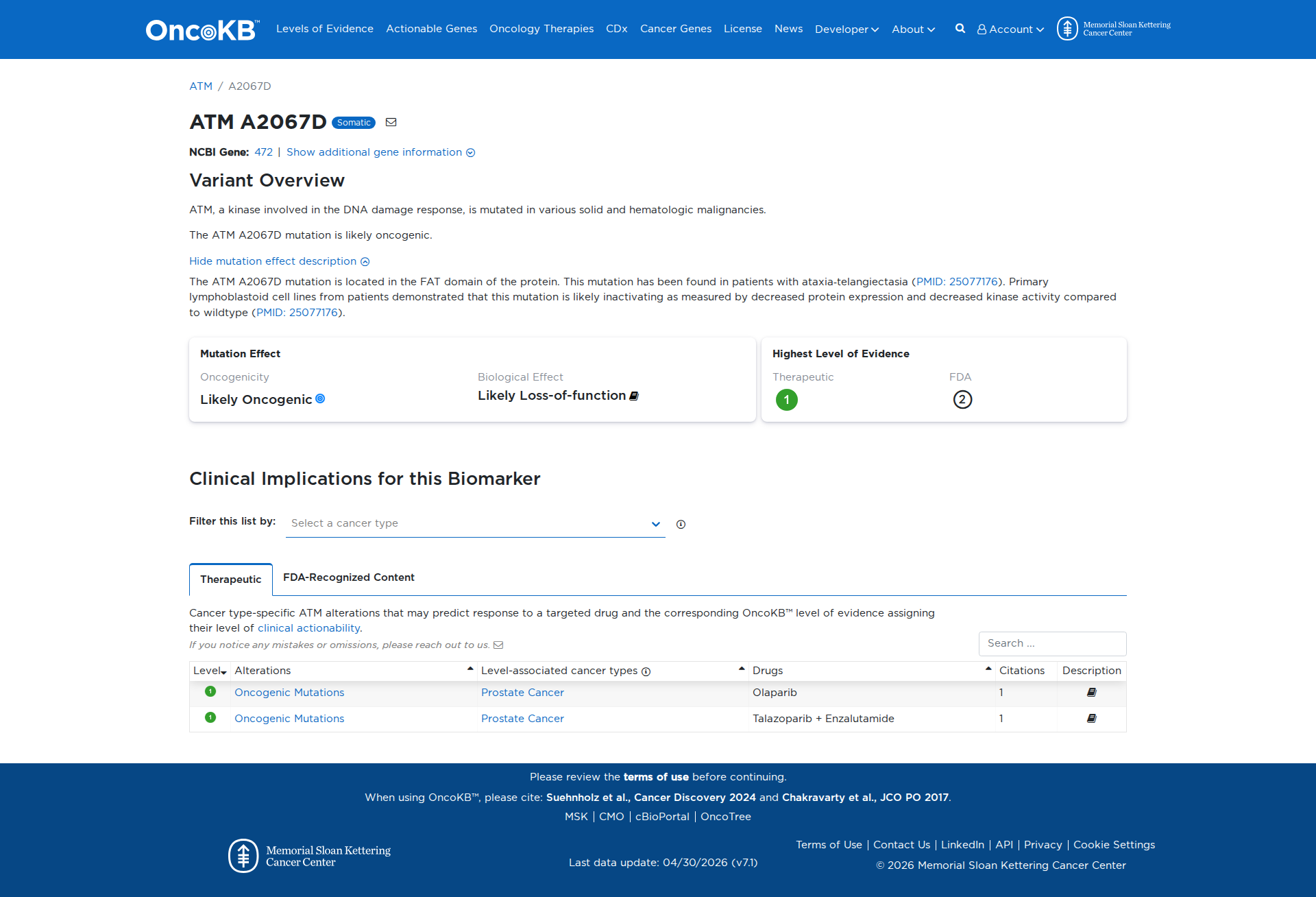
The ATM A2067D variant has been functionally characterized and demonstrates a damaging effect. It results in decreased ATM protein expression and reduced kinase activity, including loss of autophosphorylation and Smc1 phosphorylation, indicating a loss of function.
Click on previews to view full database entries. External databases may require institutional access.
Computational Analysis
Pathogenicity Predictions
SpliceAISpliceAI Scores
Window: ±500bp| Effect Type | Score | Position |
|---|---|---|
| Acceptor Loss (AL) | 0.0 | -1 bp |
| Donor Loss (DL) | 0.0 | -298 bp |
| Acceptor Gain (AG) | 0.01 | 8 bp |
| Donor Gain (DG) | 0.0 | 147 bp |
VCEP Guidelines
Applied ACMG/AMP Criteria (VCEP Specific)
PVS1 (Not Applied)
According to VCEP guidelines, the rule for PVS1 is: "Very Strong Strength: Very Strong Use ATM PVS1 Decision Tree Modification Type: Gene-specific,Strength". The evidence for this variant shows: it is a missense change (A2067D) and not a null variant expected to undergo nonsense‐mediated decay. Therefore, this criterion is not applied.
PS1 (Not Applied)
According to VCEP guidelines, the rule for PS1 is: "Strong Strength: Strong Use for protein changes as long as splicing is ruled-out for both alterations." The evidence for this variant shows: this amino acid change is novel and not previously observed via a different nucleotide change at the same codon. Therefore, this criterion is not applied.
PS2 (Not Applied)
According to standard ACMG guidelines, the rule for PS2 is: "De novo (both maternity and paternity confirmed) in a patient with the disease and no family history." The evidence for this variant shows: no information on de novo occurrence or parental genotype confirmation. Therefore, this criterion is not applied.
PS3 (Supporting)
According to VCEP guidelines, the rule for PS3 is: "Supporting Strength: Supporting Use when a variant fails to rescue an ATM specific feature, only (e.g. phosphorylation of ATM-specific targets)." The evidence for this variant shows: functional studies demonstrate decreased ATM protein expression, loss of autophosphorylation, and loss of Smc1 phosphorylation. Therefore, this criterion is applied at Supporting strength because the variant fails to rescue ATM-specific functional features.
PS4 (Not Applied)
According to VCEP guidelines, the rule for PS4 is: "Strong Strength: Case-control studies; p-value ≤ .05 AND OR ≥2; Moderate Strength: Do not use for proband counting." The evidence for this variant shows: no case-control or cohort data reported. Therefore, this criterion is not applied.
PM1 (Not Applied)
According to standard ACMG guidelines, the rule for PM1 is: "Located in a mutational hot spot and/or critical and well-established functional domain without benign variation." The evidence for this variant shows: A2067D is not located in a defined ATM hotspot or critical functional domain. Therefore, this criterion is not applied.
PM2 (Supporting)
According to VCEP guidelines, the rule for PM2 is: "Supporting Strength: Frequency ≤.001% if n=1 in a single subpopulation, that is sufficiently rare and PM2_supporting would apply." The evidence for this variant shows: MAF=0.00088% in the European (non-Finnish) population (1/113,682 alleles). Therefore, this criterion is applied at Supporting strength because the allele frequency meets the ≤.001% threshold with a single observation.
PM3 (Not Applied)
According to VCEP guidelines, the rule for PM3 is: "Use ATM PM3/BP2 table for allelic data in recessive conditions." The evidence for this variant shows: no evidence of trans configuration or recessive inheritance data. Therefore, this criterion is not applied.
PM4 (Not Applied)
According to standard ACMG guidelines, the rule for PM4 is: "Protein length changes due to in-frame deletions/insertions or stop-loss variants." The evidence for this variant shows: it is a missense substitution, not an in-frame indel or stop-loss. Therefore, this criterion is not applied.
PM5 (Not Applied)
According to VCEP guidelines, the rule for PM5 is: "Supporting Strength: Use for genomic frameshift and truncating variants with PTC upstream of p.R3047." The evidence for this variant shows: it is a missense change, not a truncating variant. Therefore, this criterion is not applied.
PM6 (Not Applied)
According to standard ACMG guidelines, the rule for PM6 is: "Assumed de novo, but without confirmation of paternity and maternity." The evidence for this variant shows: no information on de novo status or parental confirmation. Therefore, this criterion is not applied.
PP1 (Not Applied)
According to standard ACMG guidelines, the rule for PP1 is: "Co-segregation with disease in multiple affected family members." The evidence for this variant shows: no segregation data in families. Therefore, this criterion is not applied.
PP2 (Not Applied)
According to standard ACMG guidelines, the rule for PP2 is: "Missense variant in a gene with low rate of benign missense variation and where missense is a common mechanism of disease." The evidence for this variant shows: ATM has both loss‐of‐function and missense pathogenic variants, but there is insufficient evidence to consider missense the sole mechanism. Therefore, this criterion is not applied.
PP3 (Not Applied)
According to VCEP guidelines, the rule for PP3 is: "Supporting Strength: Protein: REVEL >.7333; RNA: At least one well-established in silico predictor shows impact on splicing." The evidence for this variant shows: mixed in silico predictions, no REVEL score provided, SpliceAI score 0.01 (no splicing impact). Therefore, this criterion is not applied.
PP4 (Not Applied)
According to standard ACMG guidelines, the rule for PP4 is: "Patient’s phenotype or family history is highly specific for a disease with a single genetic etiology." The evidence for this variant shows: no phenotype or clinical presentation data provided. Therefore, this criterion is not applied.
PP5 (Supporting)
According to standard ACMG guidelines, the rule for PP5 is: "Reputable source recently reports variant as pathogenic, but the evidence is not available to the laboratory to perform an independent evaluation." The evidence for this variant shows: ClinVar entries from 17 clinical laboratories classify as Likely Pathogenic or Pathogenic. Therefore, this criterion is applied at Supporting strength because multiple reputable sources report pathogenicity.
BA1 (Not Applied)
According to VCEP guidelines, the rule for BA1 is: "Stand Alone Strength: Filtering Allele Frequency >.5%." The evidence for this variant shows: allele frequency is 0.00088%, well below 0.5%. Therefore, this criterion is not applied.
BS1 (Not Applied)
According to VCEP guidelines, the rule for BS1 is: "Strong Strength: Filtering Allele Frequency >.05%." The evidence for this variant shows: allele frequency is 0.00088%, below 0.05%. Therefore, this criterion is not applied.
BS2 (Not Applied)
According to standard ACMG guidelines, the rule for BS2 is: "Observed in a healthy adult individual for a recessive (homozygous) phenotype, or observed as heterozygote with no phenotype." The evidence for this variant shows: no data on healthy individuals. Therefore, this criterion is not applied.
BS3 (Not Applied)
According to VCEP guidelines, the rule for BS3 is: "Moderate Strength: Use when a variant rescues both an ATM specific feature AND radiosensitivity; Supporting Strength: Use when a variant rescues either one." The evidence for this variant shows: functional studies demonstrate damaging effects, not rescue. Therefore, this criterion is not applied.
BS4 (Not Applied)
According to standard ACMG guidelines, the rule for BS4 is: "Lack of segregation in affected members of a family." The evidence for this variant shows: no segregation data. Therefore, this criterion is not applied.
BP1 (Not Applied)
According to standard ACMG guidelines, the rule for BP1 is: "Missense variant in a gene for which primarily truncating variants are known to cause disease." The evidence for this variant shows: ATM has both truncating and missense pathogenic variants. Therefore, this criterion is not applied.
BP2 (Not Applied)
According to VCEP guidelines, the rule for BP2 is: "Use ATM PM3/BP2 table for allelic data in recessive conditions." The evidence for this variant shows: no trans or cis allelic context data. Therefore, this criterion is not applied.
BP3 (Not Applied)
According to standard ACMG guidelines, the rule for BP3 is: "In-frame deletions/insertions in a repetitive region without a known function." The evidence for this variant shows: it is a single amino acid substitution not in a repetitive region. Therefore, this criterion is not applied.
BP4 (Not Applied)
According to VCEP guidelines, the rule for BP4 is: "Supporting Strength: Protein Analysis: REVEL score ≤.249; RNA: At least one predictor shows splicing impact." The evidence for this variant shows: no REVEL score provided, mixed in silico predictions, SpliceAI shows no splicing impact. Therefore, this criterion is not applied.
BP5 (Not Applied)
According to standard ACMG guidelines, the rule for BP5 is: "Variant found in a case with an alternate molecular basis for disease." The evidence for this variant shows: no such case data. Therefore, this criterion is not applied.
BP6 (Not Applied)
According to standard ACMG guidelines, the rule for BP6 is: "Reputable source reports variant as benign, but evidence is not available." The evidence for this variant shows: no reputable source reporting as benign. Therefore, this criterion is not applied.
BP7 (Not Applied)
According to standard ACMG guidelines, the rule for BP7 is: "Synonymous variant with no predicted splice impact and not in a splice consensus region." The evidence for this variant shows: it is a missense change. Therefore, this criterion is not applied.