Genetic Information
Gene & Transcript Details
| ID | Status | Details |
|---|---|---|
| NM_001042492.3 | MANE Select | 12373 nt | 334–8853 |
| NM_001042492.1 | Alternative | 12394 nt | 334–8853 |
| NM_001042492.2 | RefSeq Select | 12444 nt | 384–8903 |
Variant Details
Clinical & Population Data
Population Frequency
gnomADClinVar
OpenThe p.Q209* pathogenic mutation (also known as c.625C>T), located in coding exon 6 of the NF1 gene, results from a C to T substitution at nucleotide position 625. This changes the amino acid from a glutamine to a stop codon within coding exon 6. <span data-redactor="verified" style="background-color: initial;">Since premature stop codons are typically deleterious in nature, this alteration is interpreted as a disease-causing mutation (ACMG Recommendations for Standards for Interpretation and Reporting of Sequence Variations. Revision 2007. Genet Med. 2008;10:294).
This sequence change creates a premature translational stop signal (p.Gln209*) in the NF1 gene. It is expected to result in an absent or disrupted protein product. Loss-of-function variants in NF1 are known to be pathogenic (PMID: 10712197, 23913538). This variant is not present in population databases (gnomAD no frequency). This premature translational stop signal has been observed in individual(s) with neurofibromatosis, type 1 (PMID: 25480383, 26380986). Invitae Evidence Modeling of clinical and family history, age, sex, and reported ancestry of multiple individuals with this NF1 variant has been performed. This variant is expected to be pathogenic with a positive predictive value of at least 99%. This is a validated machine learning model that incorporates the clinical features of 1,785,918 individuals referred to our laboratory for NF1 testing. ClinVar contains an entry for this variant (Variation ID: 187069). For these reasons, this variant has been classified as Pathogenic.
"This variant has been reported in ClinVar as Pathogenic (4 clinical laboratories)."
COSMIC Somatic Evidence
Open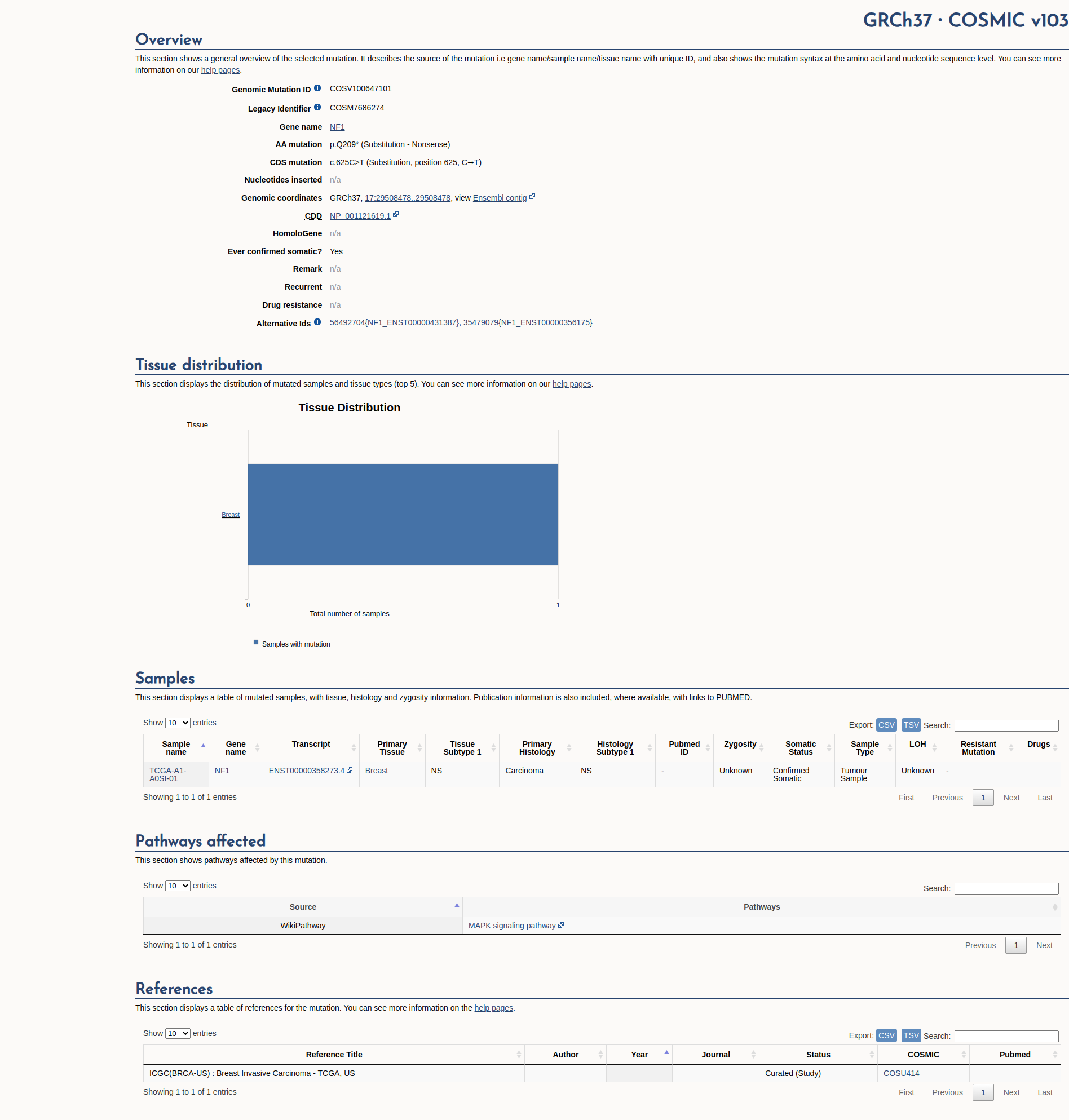
Functional Impact & Domains
Functional Domain
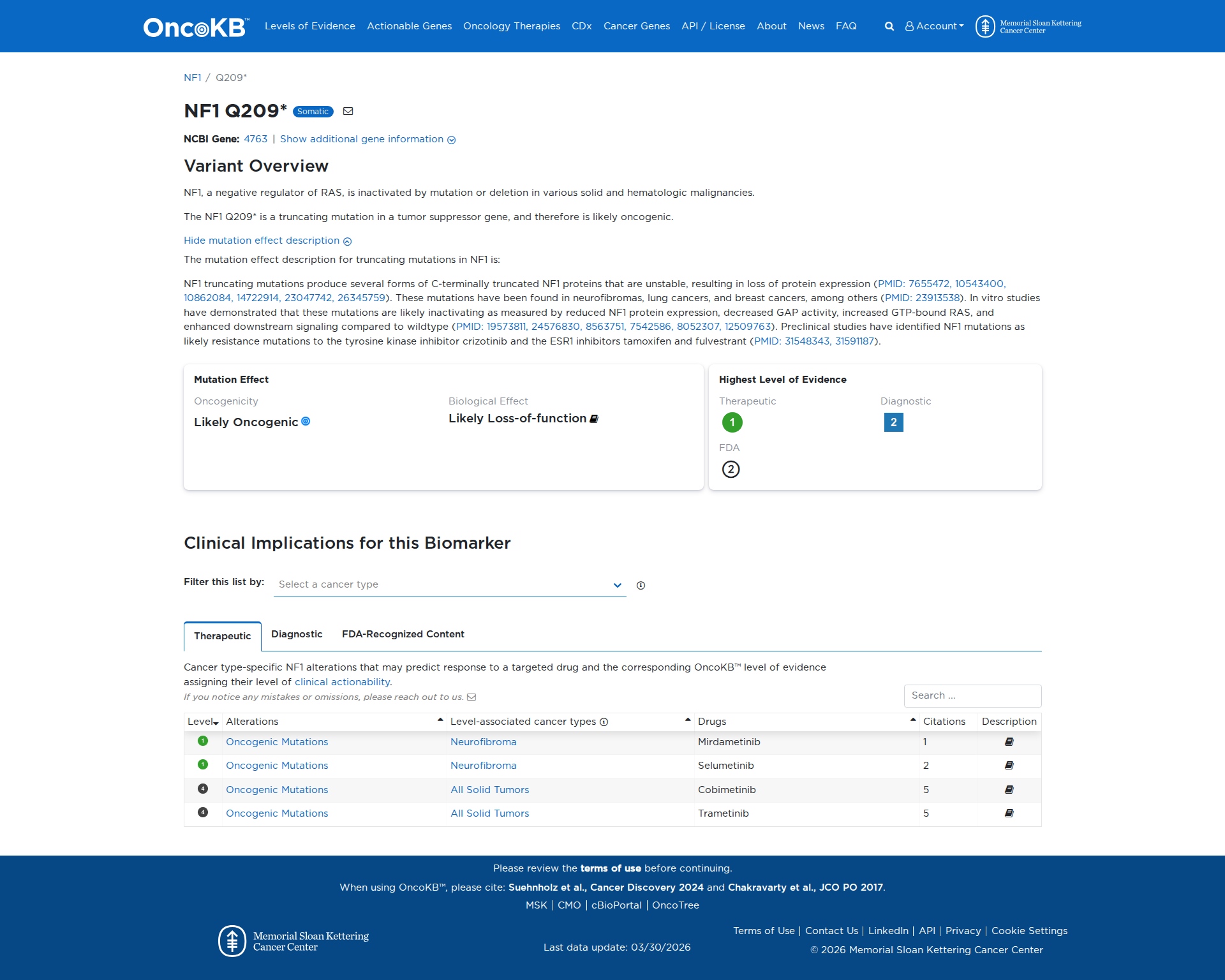
The NF1 Q209* variant is a truncating mutation in the NF1 gene, which functions as a tumor suppressor. Functional studies indicate that this mutation results in the production of unstable, C-terminally truncated NF1 proteins, leading to a loss of protein expression. This inactivation is evidenced by reduced NF1 protein levels, decreased GAP activity, increased GTP-bound RAS, and enhanced downstream signaling. These findings support the conclusion that the NF1 Q209* variant has a damaging effect, contributing to oncogenic processes.
Click on previews to view full database entries. External databases may require institutional access.
Computational Analysis
Pathogenicity Predictions
SpliceAISpliceAI Scores
Window: ±500bp| Effect Type | Score | Position |
|---|---|---|
| Acceptor Loss (AL) | 0.07 | -32 bp |
| Donor Loss (DL) | 0.02 | 29 bp |
| Acceptor Gain (AG) | 0.0 | 250 bp |
| Donor Gain (DG) | 0.0 | 325 bp |
VCEP Guidelines
Applied ACMG/AMP Criteria (VCEP Specific)
PVS1 (Very Strong)
According to standard ACMG guidelines, the rule for PVS1 is: "Null variant (nonsense, frameshift, canonical +/-1 or 2 splice sites, start loss, single exon or multiexon deletion) in a gene where loss of function is a known mechanism of disease." The evidence for this variant shows: NM_001042492.2:c.625C>T introduces a premature stop codon (p.Q209*), resulting in a null allele in NF1, a gene in which loss of function is established as a disease mechanism. Therefore, this criterion is applied at Very Strong strength because the variant is a null variant in a gene with known LOF disease mechanism.
PS1 (Not Applied)
According to standard ACMG guidelines, the rule for PS1 is: "Same amino acid change as an established pathogenic variant regardless of nucleotide change." The evidence for this variant shows: there is no other nucleotide change known to produce the same p.Q209* stop codon. Therefore, this criterion is not applied.
PS2 (Not Applied)
According to standard ACMG guidelines, the rule for PS2 is: "De novo (both maternity and paternity confirmed) in a patient with the disease and no family history." The evidence for this variant shows: parental testing and de novo status are unknown. Therefore, this criterion is not applied.
PS3 (Strong)
According to standard ACMG guidelines, the rule for PS3 is: "Well-established in vitro or in vivo functional studies supportive of a damaging effect on the gene or gene product." The evidence for this variant shows: functional studies demonstrate that p.Q209* produces unstable truncated NF1 protein, loss of NF1 expression, decreased GAP activity, increased GTP-bound RAS, and enhanced downstream signaling. Therefore, this criterion is applied at Strong strength because multiple well-established functional assays show a damaging effect.
PS4 (Not Applied)
According to standard ACMG guidelines, the rule for PS4 is: "The prevalence of the variant in affected individuals is significantly increased compared with controls." The evidence for this variant shows: no case–control or cohort data are available to demonstrate increased prevalence. Therefore, this criterion is not applied.
PM1 (Not Applied)
According to standard ACMG guidelines, the rule for PM1 is: "Located in a mutational hot spot and/or critical and well-established functional domain without benign variation." The evidence for this variant shows: no data indicating that codon 209 lies within a mutational hotspot or critical domain beyond LOF. Therefore, this criterion is not applied.
PM2 (Moderate)
According to standard ACMG guidelines, the rule for PM2 is: "Absent from controls (or at extremely low frequency if recessive) in population databases." The evidence for this variant shows: it is not present in gnomAD, ExAC, 1000 Genomes, or ESP. Therefore, this criterion is applied at Moderate strength because the variant is absent from large population datasets.
PM3 (Not Applied)
According to standard ACMG guidelines, the rule for PM3 is: "For recessive disorders, detected in trans with a pathogenic variant." The evidence for this variant shows: NF1 is autosomal dominant and there is no trans data. Therefore, this criterion is not applied.
PM4 (Not Applied)
According to standard ACMG guidelines, the rule for PM4 is: "Protein length changes due to in-frame deletions/insertions or stop-loss variants." The evidence for this variant shows: c.625C>T is a stop-gain (nonsense) variant, not an in-frame indel or stop-loss. Therefore, this criterion is not applied.
PM5 (Not Applied)
According to standard ACMG guidelines, the rule for PM5 is: "Novel missense change at an amino acid residue where a different missense change determined to be pathogenic has been seen before." The evidence for this variant shows: this is a nonsense variant, not missense. Therefore, this criterion is not applied.
PM6 (Not Applied)
According to standard ACMG guidelines, the rule for PM6 is: "Assumed de novo, without confirmation of paternity and maternity." The evidence for this variant shows: de novo status is unknown. Therefore, this criterion is not applied.
PP1 (Not Applied)
According to standard ACMG guidelines, the rule for PP1 is: "Cosegregation with disease in multiple affected family members in a gene definitively known to cause the disease." The evidence for this variant shows: no family segregation data. Therefore, this criterion is not applied.
PP2 (Not Applied)
According to standard ACMG guidelines, the rule for PP2 is: "Missense variant in a gene with a low rate of benign missense variation and where missense is a common mechanism of disease." The evidence for this variant shows: it is a nonsense variant. Therefore, this criterion is not applied.
PP3 (Not Applied)
According to standard ACMG guidelines, the rule for PP3 is: "Multiple lines of computational evidence support a deleterious effect on the gene or gene product." The evidence for this variant shows: CADD score 8.58 (below pathogenic threshold), SpliceAI scores ≤0.07, and other predictors are mixed. Therefore, this criterion is not applied.
PP4 (Not Applied)
According to standard ACMG guidelines, the rule for PP4 is: "Patient’s phenotype or family history is highly specific for a disease with a single genetic etiology." The evidence for this variant shows: no clinical phenotype or family history was provided. Therefore, this criterion is not applied.
PP5 (Supporting)
According to standard ACMG guidelines, the rule for PP5 is: "Reputable source recently reports variant as pathogenic, but the evidence is not available to the laboratory to perform an independent evaluation." The evidence for this variant shows: ClinVar lists this variant as pathogenic in four independent clinical laboratory submissions. Therefore, this criterion is applied at Supporting strength because a reputable database reports pathogenicity without available primary data.
BA1 (Not Applied)
According to standard ACMG guidelines, the rule for BA1 is: "Allele frequency is greater than 5% in population databases." The evidence for this variant shows: it is absent from population databases. Therefore, this criterion is not applied.
BS1 (Not Applied)
According to standard ACMG guidelines, the rule for BS1 is: "Allele frequency is greater than expected for the disorder." The evidence for this variant shows: it is absent from population databases. Therefore, this criterion is not applied.
BS2 (Not Applied)
According to standard ACMG guidelines, the rule for BS2 is: "Observed in a healthy adult with full penetrance expected at an early age." The evidence for this variant shows: no observations in healthy individuals. Therefore, this criterion is not applied.
BS3 (Not Applied)
According to standard ACMG guidelines, the rule for BS3 is: "Well-established in vitro or in vivo functional studies show no damaging effect on protein function or splicing." The evidence for this variant shows: functional studies demonstrate damaging effect. Therefore, this criterion is not applied.
BS4 (Not Applied)
According to standard ACMG guidelines, the rule for BS4 is: "Lack of segregation in affected members of a family." The evidence for this variant shows: no segregation data provided. Therefore, this criterion is not applied.
BP1 (Not Applied)
According to standard ACMG guidelines, the rule for BP1 is: "Missense variant in a gene for which primarily truncating variants are known to cause disease." The evidence for this variant shows: it is a truncating variant. Therefore, this criterion is not applied.
BP2 (Not Applied)
According to standard ACMG guidelines, the rule for BP2 is: "Observed in trans with a pathogenic variant for a dominant disorder." The evidence for this variant shows: no trans observations. Therefore, this criterion is not applied.
BP3 (Not Applied)
According to standard ACMG guidelines, the rule for BP3 is: "In-frame deletions/insertions in a repetitive region without a known function." The evidence for this variant shows: it is a nonsense variant. Therefore, this criterion is not applied.
BP4 (Supporting)
According to standard ACMG guidelines, the rule for BP4 is: "Multiple lines of computational evidence suggest no impact on gene or gene product." The evidence for this variant shows: CADD score 8.58, SpliceAI ≤0.07, and other predictors do not support a deleterious effect. Therefore, this criterion is applied at Supporting strength because computational tools predict no functional impact.
BP5 (Not Applied)
According to standard ACMG guidelines, the rule for BP5 is: "Variant found in a case with an alternate molecular basis for disease." The evidence for this variant shows: no alternative molecular diagnosis reported. Therefore, this criterion is not applied.
BP6 (Not Applied)
According to standard ACMG guidelines, the rule for BP6 is: "Reputable source reports variant as benign but evidence not available." The evidence for this variant shows: no benign assertions in reputable sources. Therefore, this criterion is not applied.
BP7 (Not Applied)
According to standard ACMG guidelines, the rule for BP7 is: "Synonymous variant with no predicted impact on splicing." The evidence for this variant shows: it is a nonsense variant. Therefore, this criterion is not applied.