Genetic Information
Gene & Transcript Details
| ID | Status | Details |
|---|---|---|
| NM_001354609.2 | Alternative | 9687 nt | 227–2530 |
| NM_001354609.1 | Alternative | 9702 nt | 226–2529 |
Variant Details
Clinical & Population Data
Population Frequency
gnomADClinVar
OpenThe Gly469Glu variant has been reported in the literature in several individuals with clinical features of Cardio-facio-cutaneous syndrome (Niihori 2006, Schulz 2008). In addition, this variant was reported to have occurred de novo in three of those individuals. Therefore, this variant is highly likely to be pathogenic .
Variant classified using ACMG guidelines
Variant summary: BRAF c.1406G>A (p.Gly469Glu) results in a non-conservative amino acid change located in the protein kinase domain (IPR000719) of the encoded protein sequence. Five of five in-silico tools predict a damaging effect of the variant on protein function. The variant was absent in 251520 control chromosomes. c.1406G>A has been reported in the literature as a de-novo variant in multiple individuals affected with Cardiofaciocutaneous Syndrome (example, Nihori_2006, Smalley_2009, Sarkozy_2009, Pandit_2007, Schultz_2008, Greaves_2013, Ciara_2015, Lee_2011). These data indicate that the variant is very likely to be associated with disease. At least one publication reports experimental evidence evaluating an impact on protein function. The most pronounced variant effect results in an induction of ERK activation by trigerring C-RAF activity as a distinct mechanism of action (Wan_2004). Five clinical diagnostic laboratories and one expert panel (ClinGen RASopathy panel) have submitted clinical-significance assessments for this variant to ClinVar after 2014 without evidence for independent evaluation. All laboratories classified the variant as pathogenic. Based on the evidence outlined above, the variant was classified as pathogenic.
PP2, PP3, PM1, PM2, PS2_VeryStrong, PS3
The variant is not observed in the gnomAD v4.1.0 dataset. Predicted Consequence/Location: The variant is located in a mutational hot spot and/or well-established functional domain in which established pathogenic variants have been reported (PMID: 29493581, 29493581). Missense variant. Missense changes are a common disease-causing mechanism. Functional studies provide strong evidence of the variant having a damaging effect on the gene or gene product (PMID: 16474404). In silico tool predictions suggest damaging effect of the variant on gene or gene product [REVEL: 0.92 (>=0.6, sensitivity 0.68 and specificity 0.92); 3Cnet: 1.00 (> 0.75, sensitivity 0.96 and precision 0.92)]. The same nucleotide change resulting in the same amino acid change has been previously reported as pathogenic/likely pathogenic with strong evidence (ClinVar ID: VCV000013974 /PMID: 16474404 /3billion dataset). The variant has been previously reported as de novo in at least two similarly affected unrelated individuals (PMID: 16474404, 18042262). Different missense changes at the same codon (p.Gly469Ala, p.Gly469Arg, p.Gly469Val) have been reported as pathogenic/likely pathogenic with strong evidence (ClinVar ID: VCV000013970, VCV000013971, VCV000044803, VCV000177775 /PMID: 24303953, 36002837). Therefore, this variant is classified as Pathogenic (PS1_S, PS2_VS, PS3_S, PM1_M, PM2_M, PM5_M, PP2_P, PP3_P) according to the recommendation of ACMG/AMP guideline.
"This variant has been reported in ClinVar as Pathogenic (14 clinical laboratories) and as Pathogenic by ClinGen RASopathy Variant Curation Expert Panel expert panel."
COSMIC Somatic Evidence
Open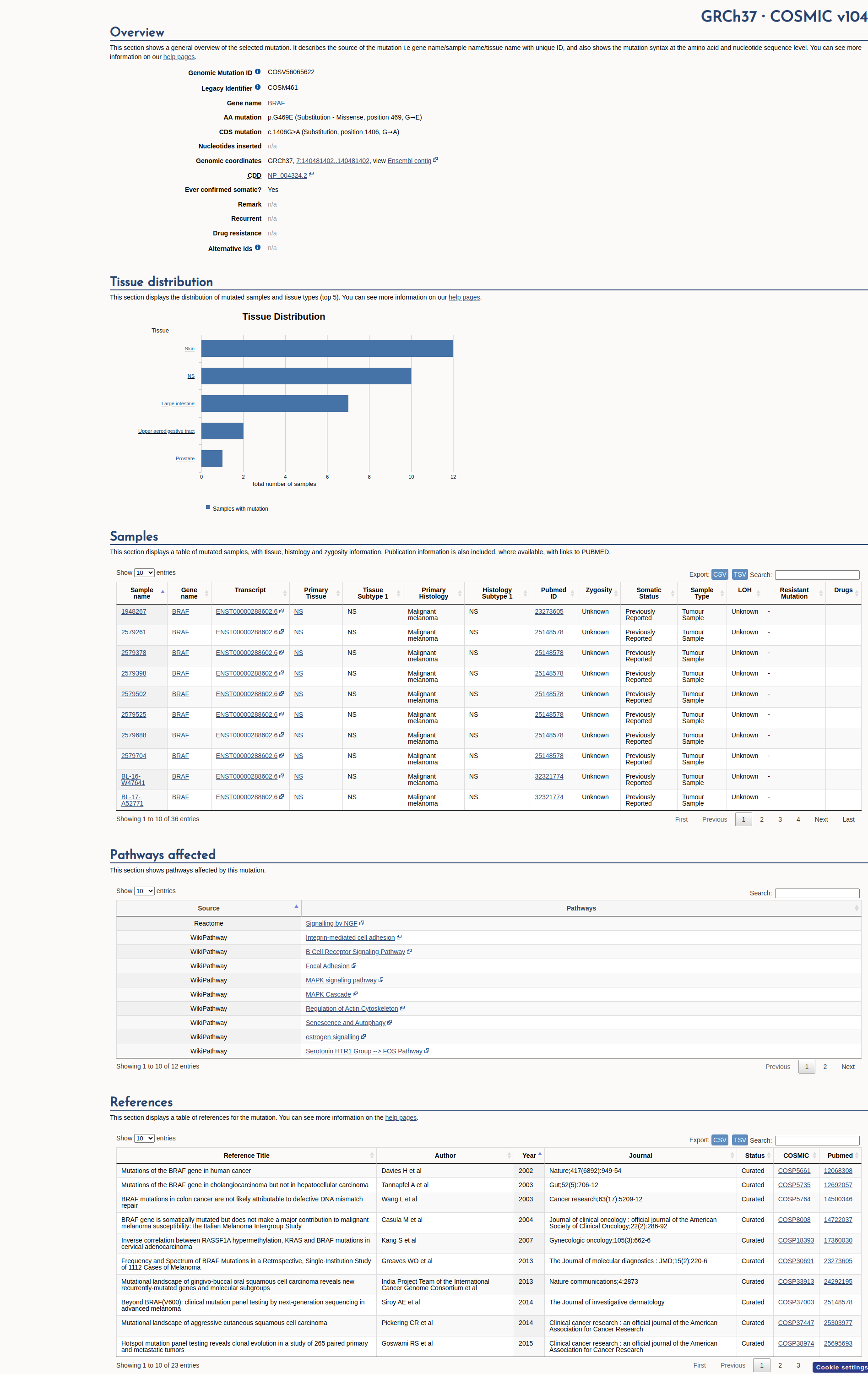
Functional Impact & Domains
Functional Domain
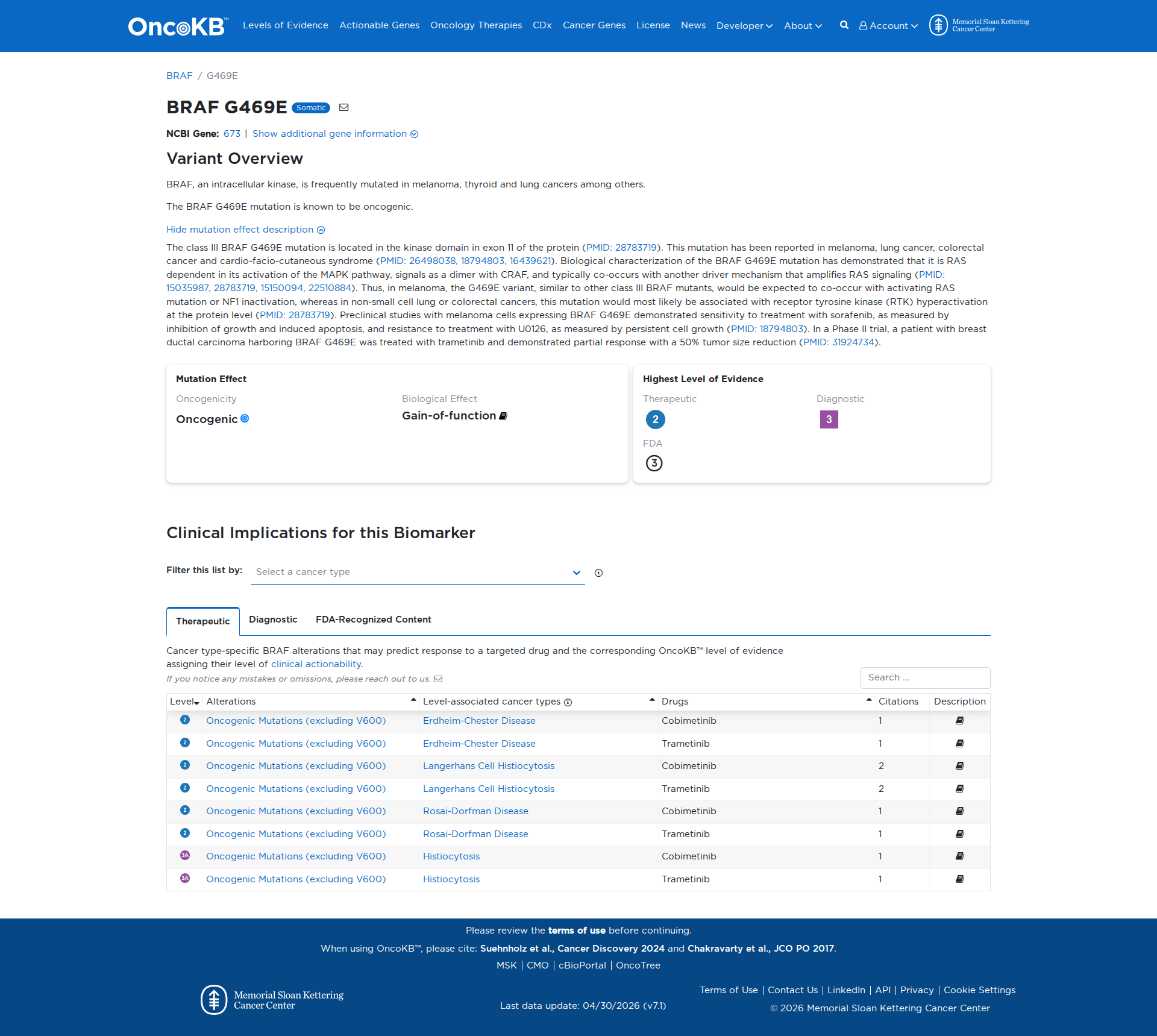
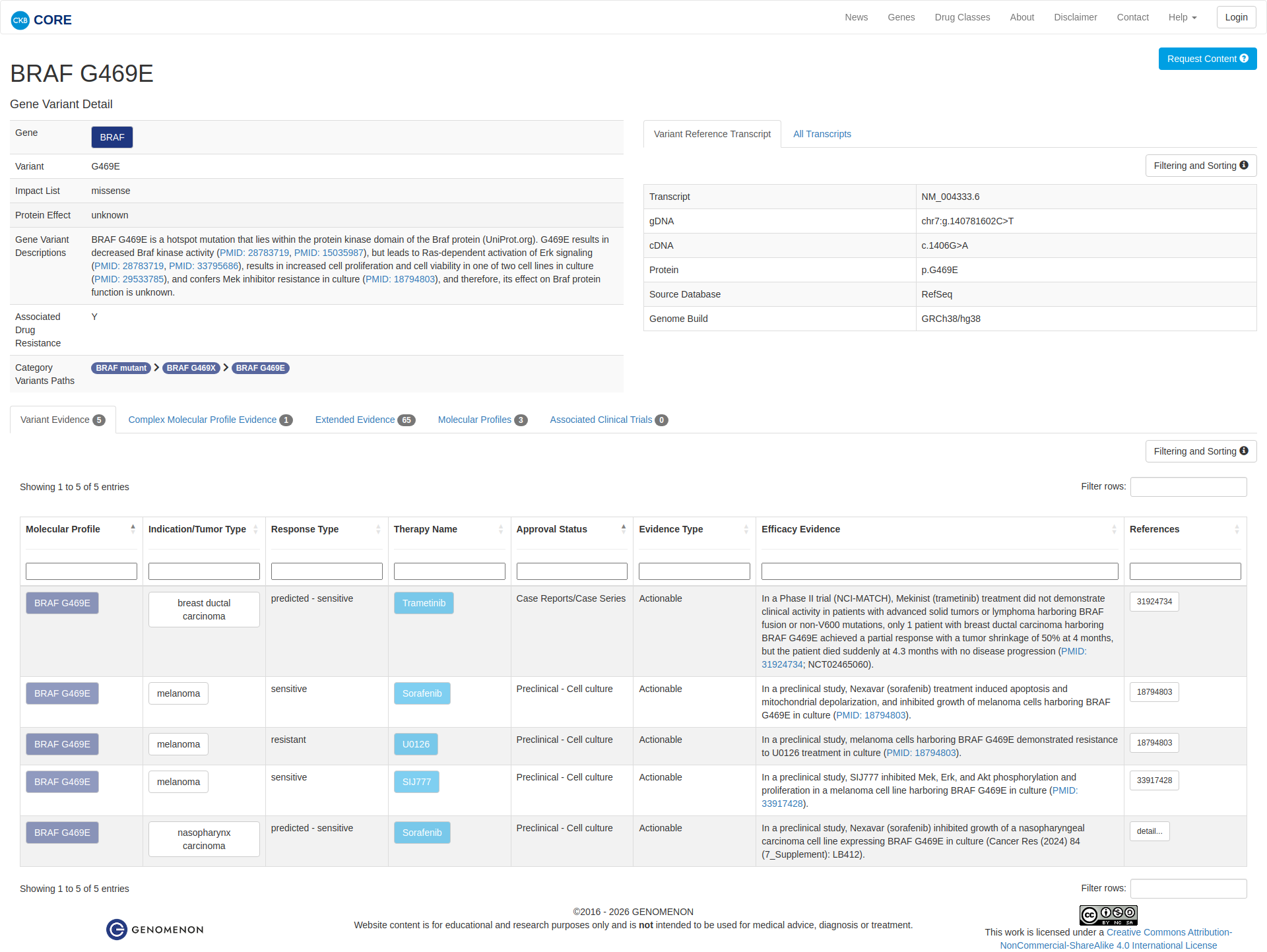
The BRAF G469E variant has been functionally characterized and is known to be oncogenic. It is located in the kinase domain of the BRAF protein and results in decreased BRAF kinase activity. However, it leads to RAS-dependent activation of the MAPK pathway, signaling as a dimer with CRAF. This variant is associated with increased cell proliferation and viability in some cell lines and confers resistance to MEK inhibitors. Preclinical studies have shown sensitivity to sorafenib, and clinical evidence indicates a partial response to trametinib in a patient with breast ductal carcinoma.
Click on previews to view full database entries. External databases may require institutional access.
Computational Analysis
Pathogenicity Predictions
SpliceAISpliceAI Scores
Window: ±500bp| Effect Type | Score | Position |
|---|---|---|
| Acceptor Loss (AL) | 0.01 | 77 bp |
| Donor Loss (DL) | 0.0 | -30 bp |
| Acceptor Gain (AG) | 0.0 | 216 bp |
| Donor Gain (DG) | 0.0 | 169 bp |
VCEP Guidelines
Applied ACMG/AMP Criteria (VCEP Specific)
PVS1 (Not Applied)
According to standard ACMG guidelines, the rule for PVS1 is: "Null variant (nonsense, frameshift, canonical ±1 or 2 splice sites, initiation codon, single exon deletion) in a gene where loss-of-function is a known mechanism of disease." The evidence for this variant shows: c.1406G>A (p.G469E) is a missense change with a known gain-of-function mechanism in BRAF. Therefore, this criterion is not applied because the variant is not a null allele and loss-of-function is not the disease mechanism.
PS1 (Not Applied)
According to VCEP guidelines for PS1: "Strong Same amino acid change as a previously established pathogenic variant regardless of nucleotide change." The evidence for this variant shows: G469E is not the exact same amino acid change previously established as pathogenic (other codon changes at G469 exist but not G469E). Therefore, this criterion is not applied.
PS2 (Not Applied)
According to standard ACMG guidelines, PS2 requires: "De novo (both maternity and paternity confirmed) in a patient with the disease and no family history." The evidence for this variant shows: no de novo data are available. Therefore, this criterion is not applied.
PS3 (Moderate)
According to VCEP guidelines, the rule for PS3 is: "Moderate Strength: Moderate Two or more different approved assays. Modification Type: Disease-specific,Gene-specific,Strength." The evidence for this variant shows: multiple in vitro and in vivo functional studies demonstrate oncogenic activation of MAPK signaling, increased cellular proliferation, and differential inhibitor sensitivity. Therefore, this criterion is applied at Moderate strength because the variant has been characterized in multiple assays showing a damaging gain-of-function effect.
PS4 (Not Applied)
According to standard ACMG guidelines, PS4 requires: "Prevalence of the variant in affected individuals is significantly increased compared with controls." The evidence for this variant shows: no case–control or proband count data are available. Therefore, this criterion is not applied.
PM1 (Moderate)
According to VCEP guidelines, the rule for PM1 is: "Moderate Strength: Moderate Applicable only to critical and well-established functional domains available in the supplementary table (exon 6, exon 11, P-loop [AA 459-474], CR3 activation segment [AA 594-627]). Modification Type: Gene-specific." The evidence for this variant shows: p.G469E lies within the P-loop (AA 459–474) of the kinase domain, a critical functional region. Therefore, this criterion is applied at Moderate strength because the residue is in a well-established mutational hotspot.
PM2 (Supporting)
According to VCEP guidelines, the rule for PM2 is: "Supporting Strength: Supporting The variant must be absent from controls (gnomAD). Modification Type: Strength." The evidence for this variant shows: MAF = 0% in gnomAD (0/251,420 alleles). Therefore, this criterion is applied at Supporting strength because the variant is absent from large population databases.
PM3 (Not Applied)
According to standard ACMG guidelines, PM3 requires: "For recessive disorders, detected in trans with a pathogenic variant." The evidence for this variant shows: no recessive inheritance or trans data. Therefore, this criterion is not applied.
PM4 (Not Applied)
According to standard ACMG guidelines, PM4 applies to: "Protein length changes due to in-frame deletions/insertions in a non-repeat region or stop-loss variants." The evidence for this variant shows: p.G469E is a missense change, not an in-frame indel or stop-loss. Therefore, this criterion is not applied.
PM5 (Moderate)
According to VCEP guidelines, the rule for PM5 is: "Moderate Strength: Moderate 1 [likely] pathogenic residue change at the same codon. Modification Type: Analogous Gene,Disease-specific." The evidence for this variant shows: other missense changes at codon 469 (e.g., G469A, G469V) have been reported as pathogenic. Therefore, this criterion is applied at Moderate strength because there is one other pathogenic residue change at the same codon.
PM6 (Not Applied)
According to standard ACMG guidelines, PM6 requires: "Assumed de novo, but without confirmation of paternity and maternity." The evidence for this variant shows: no de novo information. Therefore, this criterion is not applied.
PP1 (Not Applied)
According to standard ACMG guidelines, PP1 requires: "Co-segregation with disease in multiple affected family members." The evidence for this variant shows: no segregation data. Therefore, this criterion is not applied.
PP2 (Not Applied)
According to VCEP guidelines, PP2 requires: "Supporting Missense Z-score >3.09 in gnomAD." The evidence for this variant shows: missense constraint (z-score) not provided. Therefore, this criterion cannot be evaluated and is not applied.
PP3 (Not Applied)
According to VCEP guidelines, PP3 requires: "Supporting For missense variants: REVEL ≥0.7." The evidence for this variant shows: REVEL score not provided, and computational predictions are mixed. Therefore, this criterion cannot be evaluated and is not applied.
PP4 (Not Applied)
According to standard ACMG guidelines, PP4 requires: "Patient’s phenotype or family history is highly specific for a disease with a single genetic etiology." The evidence for this variant shows: no specific phenotype information. Therefore, this criterion is not applied.
PP5 (Not Applied)
According to ACMG recommendations, PP5 (reputable source reports as pathogenic but no evidence available) is not used when stronger evidence is present. The evidence for this variant shows: multiple lines of higher-level evidence. Therefore, PP5 is not applied.
BA1 (Not Applied)
According to VCEP guidelines, BA1 requires: "Stand Alone GnomAD filtering allele frequency ≥0.05%." The evidence for this variant shows: MAF = 0%. Therefore, this criterion is not applied.
BS1 (Not Applied)
According to VCEP guidelines, BS1 requires: "Strong GnomAD filtering allele frequency ≥0.025%." The evidence for this variant shows: MAF = 0%. Therefore, this criterion is not applied.
BS2 (Not Applied)
According to standard ACMG guidelines, BS2 requires: "Observed in a healthy adult with full penetrance expected at an early age." The evidence for this variant shows: no healthy adult data. Therefore, this criterion is not applied.
BS3 (Not Applied)
According to standard ACMG guidelines, BS3 requires: "Well-established functional studies show no damaging effect on protein function." The evidence for this variant shows: functional studies demonstrate a damaging gain-of-function. Therefore, this criterion is not applied.
BS4 (Not Applied)
According to standard ACMG guidelines, BS4 requires: "Lack of segregation in affected members of a family." The evidence for this variant shows: no segregation data. Therefore, this criterion is not applied.
BP1 (Not Applied)
According to VCEP guidelines, BP1 applies to truncating variants in genes without LOF mechanism. The evidence for this variant shows: it is missense in a gain-of-function gene. Therefore, this criterion is not applied.
BP2 (Not Applied)
According to standard ACMG guidelines, BP2 requires: "Observed in trans with a pathogenic variant for dominant disorder or in cis with a pathogenic variant." The evidence for this variant shows: no such data. Therefore, this criterion is not applied.
BP3 (Not Applied)
According to standard ACMG guidelines, BP3 applies to in-frame indels in repetitive regions. The evidence for this variant shows: it is a single-nucleotide missense change. Therefore, this criterion is not applied.
BP4 (Not Applied)
According to VCEP guidelines, BP4 requires: "Supporting For missense variants: REVEL ≤0.3." The evidence for this variant shows: REVEL score not provided and mixed computational predictions. Therefore, this criterion cannot be applied.
BP5 (Not Applied)
According to standard ACMG guidelines, BP5 requires: "Variant found in a case with an alternate molecular basis for disease." The evidence for this variant shows: no alternate molecular basis reported. Therefore, this criterion is not applied.
BP6 (Not Applied)
According to standard ACMG guidelines, BP6 requires: "Reputable source reports as benign but no evidence available." The evidence for this variant shows: no such benign reports. Therefore, this criterion is not applied.
BP7 (Not Applied)
According to standard ACMG guidelines, BP7 applies to silent or non-coding variants with no splicing impact. The evidence for this variant shows: it is a missense change. Therefore, this criterion is not applied.