c.507G>A is a silent (synonymous) substitution in BRCA1 exon 7 producing p.Gln169= (NP_009225.1:p.(Q169=)). BP1_Strong is met: the variant is a silent substitution at residue 169, which is outside all three BRCA1 clinically important functional domains (RING aa2-101, coiled-coil aa1391-1424, BRCT repeats aa1650-1857), and SpliceAI predicts no splicing impact (max delta 0.01).1 The variant is present at very low frequency in gnomAD population databases (v2.1: 3/282870 alleles; v4.1: 28/1613772 alleles) but does not meet BS1 or BA1 thresholds.2 PVS1, PS1, PS5, PM5, and BP4 are not applicable due to the silent nature of the variant. PP3 is not met (SpliceAI 0.01 < 0.2). PM2 is not met (variant is present in gnomAD).3 PS3, BS3, and BP7 remain not assessed pending verification of a reported minigene splicing assay (Fraile-Bethencourt et al. 2017) that found no splicing aberration. Confirmation of this finding would support BS3 and BP7. PP4 and BP5 are not assessed because the variant is not represented in the Li et al. 2020 (PMID:31853058) clinical-history likelihood ratio table or the Parsons et al. 2019 multifactorial dataset.4 ClinVar reports an ENIGMA expert panel classification of Likely benign (ClinVar ID 185706, review status: reviewed by expert panel). The ENIGMA classification likely incorporates the minigene splicing evidence and/or additional clinical data not captured in the available VCEP spreadsheets.5 Under strict ENIGMA Table 3 combining rules, BP1_Strong alone is insufficient to reach Likely Benign without at least one additional supporting benign criterion of a different evidence type. The available data therefore place this variant between Likely Benign (per ENIGMA expert panel classification) and VUS (per strict criteria-based adjudication without verified BS3/BP7).6
BRCA1
Final classification
Likely Benign
BRCA1 c.507G>A · p.Gln169=
BRCA1
c.507G>A is a silent (synonymous) substitution in BRCA1 exon 7 producing p.Gln169= (NP_009225.1:p.(Q169=)).
ENIGMA Table 3: 1 Strong (Benign) + 1 Supporting (Benign) = Likely Benign. Point score: -5 (range -6 to -2).
Classification rationale
BP1BP6
Likely Benign
BRCA1 c.507G>A
BP1 + BP6
→
Likely Benign
4
vcep_pmid_31853058_brca1_clinical_history_lrvcep_humu_40_1557_s001
Gene diagram
· NM_007294.4 · variants mapped to exon structure
BRCA1
NM_007294.4
Fetching transcript structure from UCSC…
Applied criteria · 2 applied · 14 assessed
Applied · 2
Strength
Supporting
Moderate
Strong
Very strong
✓
BP1
strong
Benign
ENIGMA BP1_Strong applies to silent substitutions outside a (potentially) clinically important functional domain with no predicted splicing impact (SpliceAI ≤0.1). c.507G>A is a silent variant (p.Gln169=). Residue 169 is outside all three BRCA1 clinically important functional domains (RING aa2-101, coiled-coil aa1391-1424, BRCT repeats aa1650-1857). SpliceAI max delta score is 0.01, well below the 0.1 threshold. All conditions for BP1_Strong are satisfied.
Silent variant p.Gln169= at residue 169outside all BRCA1 functional domains (RING aa2-101coiled-coil aa1391-1424
Assessed · not applied
Pathogenic
PS3
c.507G>A is not listed in ENIGMA Specifications Table 9 (calibrated functional assay results).
PS4
No case-control study demonstrating statistically significant enrichment of c.507G>A in affected individuals compared to controls was identified.
PM2
ENIGMA PM2_Supporting requires the variant to be absent from gnomAD v2.1 (non-cancer, exome only) and gnomAD v3.1 (non-cancer) outbred populations.
PP1
No co-segregation data are available for c.507G>A.
PP3
ENIGMA PP3 applies to silent variants only when SpliceAI ≥0.2, indicating a predicted splicing impact.
PP4
c.507G>A is not listed in the Li et al.
Benign
BA1
ENIGMA BA1 requires filter allele frequency (FAF) above 0.1% (FAF > 0.001) in gnomAD v2.1 (non-cancer, exome only) and/or gnomAD v3.1 (non-cancer), non-founder populations.
BS1
ENIGMA BS1_Strong requires FAF > 0.0001 (0.01%), and BS1_Supporting requires FAF > 0.00002 (0.002%) and ≤ 0.0001 in gnomAD non-cancer non-founder populations.
BS2
ENIGMA BS2 is applied in the absence of Fanconi Anemia phenotype features, using a points-based system per Specifications Table 8.
BS3
c.507G>A is not listed in ENIGMA Specifications Table 9, which assigns calibrated PS3/BS3 codes based on published functional assay results.
BS4
No lack-of-segregation data are available for c.507G>A.
BP4
ENIGMA BP4_Supporting for silent variants applies only when the variant is located inside a (potentially) clinically important functional domain and SpliceAI ≤0.1.
BP5
c.507G>A is not listed in the Li et al.
BP7
ENIGMA BP7_Strong (RNA) requires well-established mRNA assay evidence showing no damaging effect on splicing.
N/A · 12
PVS1 · PS1 · PS2 · PM1 · PM3 · PM4 · PM5 · PM6 · PP2 · PP5 · BP2 · BP3
Research & evidence
Population frequency · supports benign
gnomAD v4.1
gnomAD v2.1
v4.1
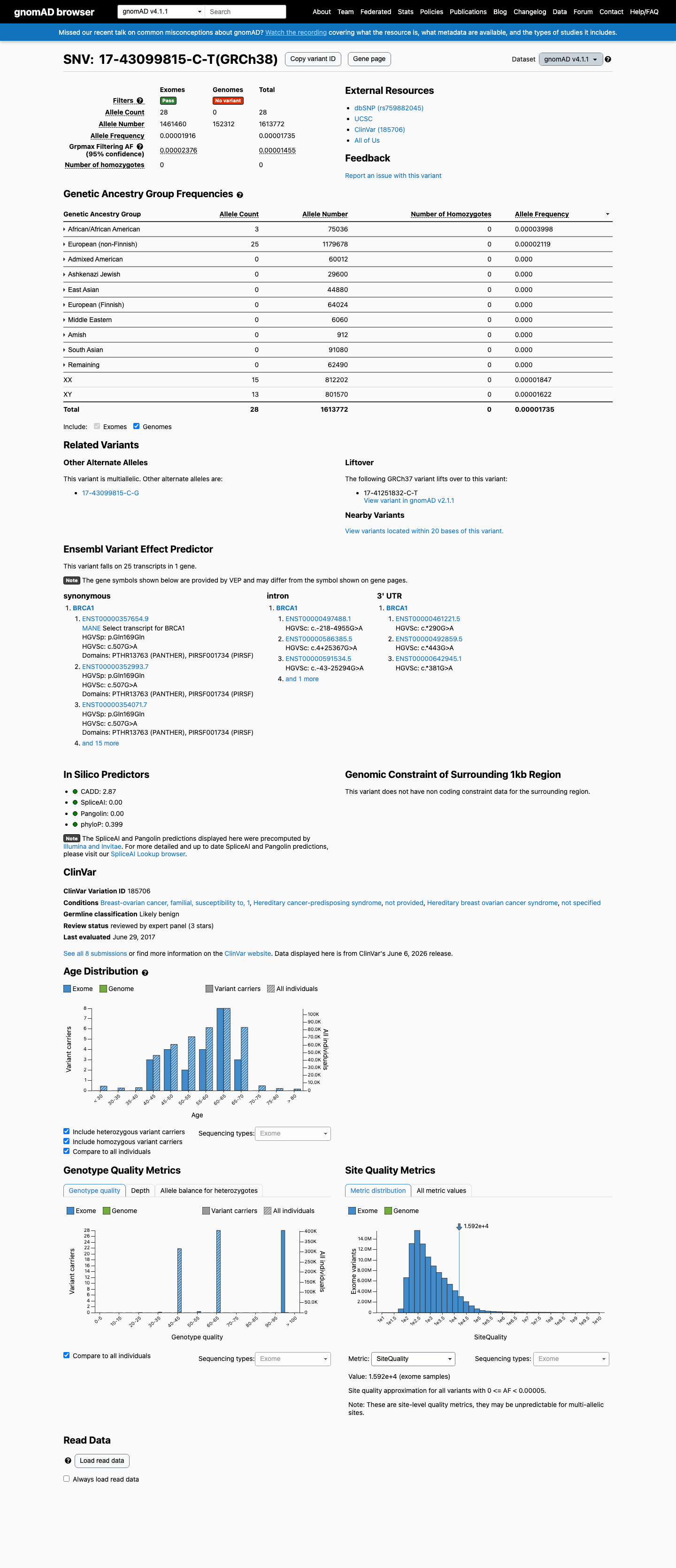
This variant is present in gnomAD v4.1 (AF= 1.73507e-05; MAF= 0.00174%, 28/1613772 alleles, homozygotes = 0) and has highest observed frequency in the African/African American population (AF= 3.99808e-05; MAF= 0.00400%, 3/75036 alleles, homozygotes = 0); grpmax FAF= 1.455e-05.
v2.1
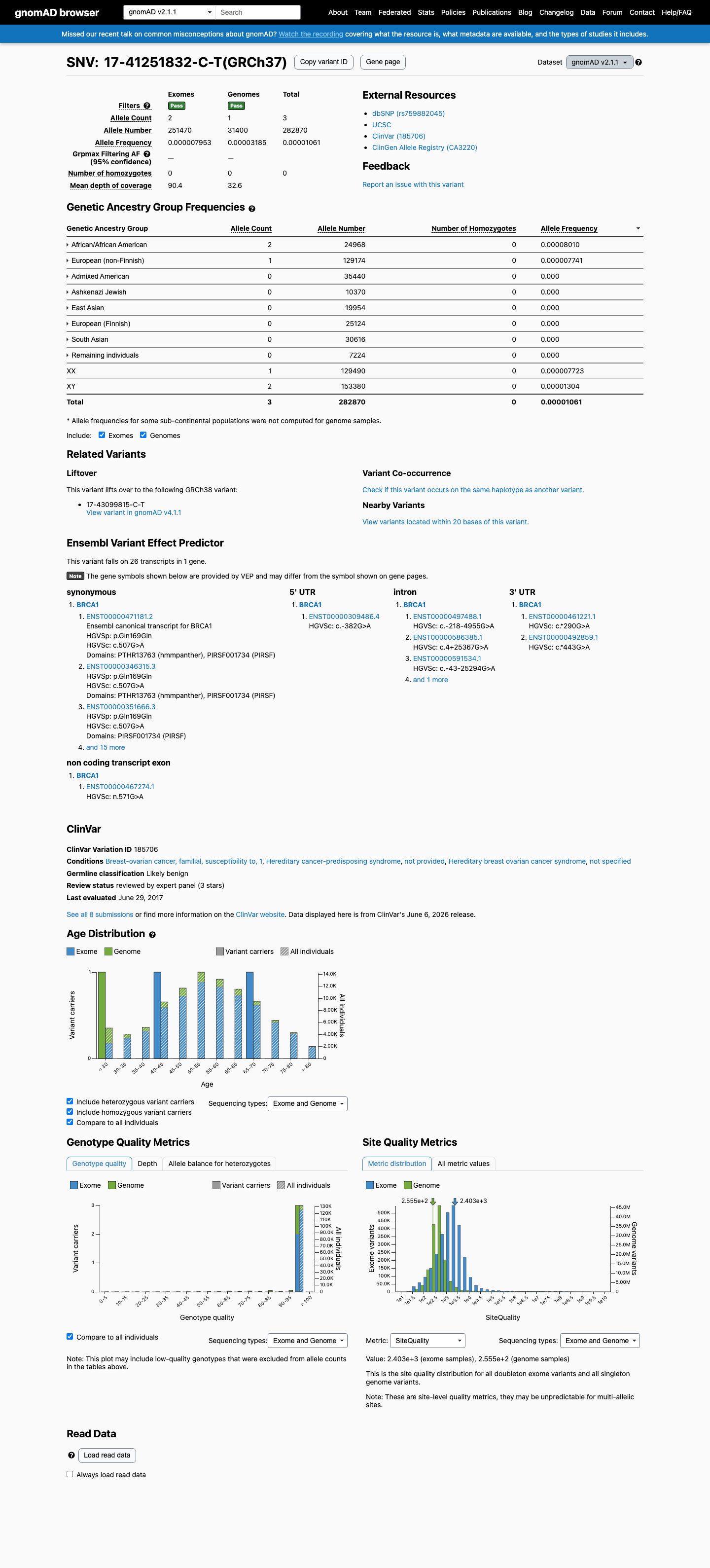
This variant is present in gnomAD v2.1 (AF= 1.06056e-05; MAF= 0.00106%, 3/282870 alleles, homozygotes = 0) and has highest observed frequency in the African/African American population (AF= 8.01025e-05; MAF= 0.00801%, 2/24968 alleles, homozygotes = 0).
🇨🇦 CA
This variant is absent from gnomAD-Canada.
Allele frequency by ancestry
three datasets · side by side
gnomAD v4.1
0.0017%
· 28 / 1,613,772
0 hom · FAF 0.0015%
0 hom · FAF 0.0015%
African/African American 3 / 75,036 |
0.004% |
European (non-Finnish) 25 / 1,179,678 |
0.0021% |
+ 8 not observed (Remaining individuals, Admixed American, European (Finnish), Amish, East Asian, Middle Eastern, South Asian, Ashkenazi Jewish)
gnomAD v2.1
0.0011%
· 3 / 282,870
0 hom
0 hom
African/African American 2 / 24,968 |
0.008% |
European (non-Finnish) 1 / 129,174 |
0.00077% |
+ 6 not observed (Admixed American, Ashkenazi Jewish, East Asian, European (Finnish), Remaining individuals, South Asian)
gnomAD Canada 🇨🇦
Absent
· 0 / ?
0 hom
0 hom
Not observed in any ancestry group.
ClinVar
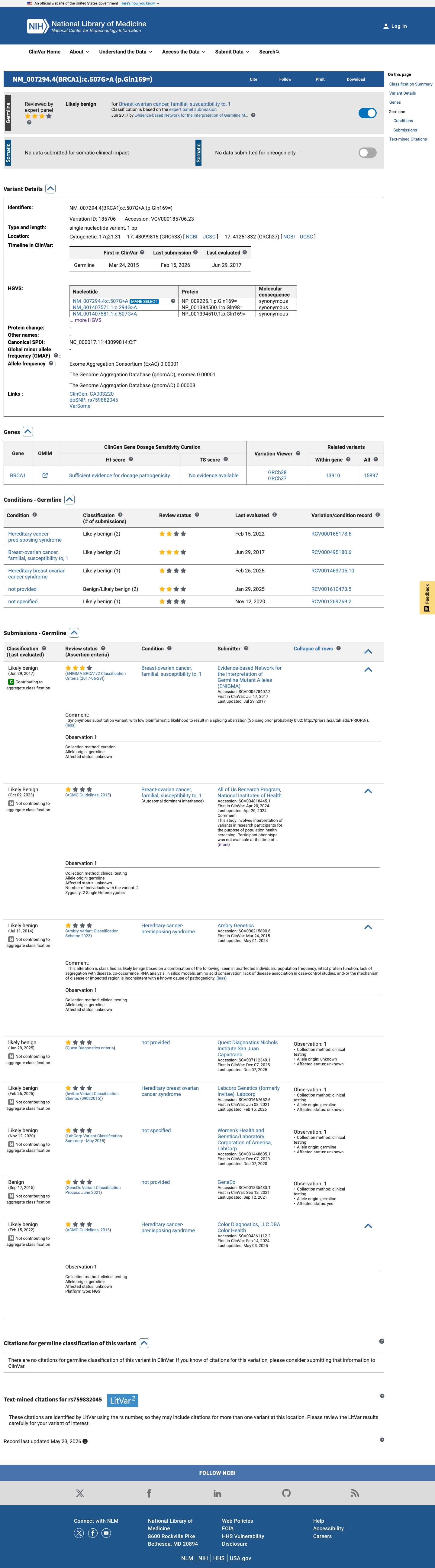
This variant has been reported in ClinVar as Likely benign (4 clinical laboratories) and as Likely Benign (1 clinical laboratory) and as likely benign (1 clinical laboratory) and as Benign (1 clinical laboratory) and as Likely benign by Evidence-based Network for the Interpretation of Germline Mutant Alleles (ENIGMA) (expert panel). (ClinVarID = 185706)
In silico
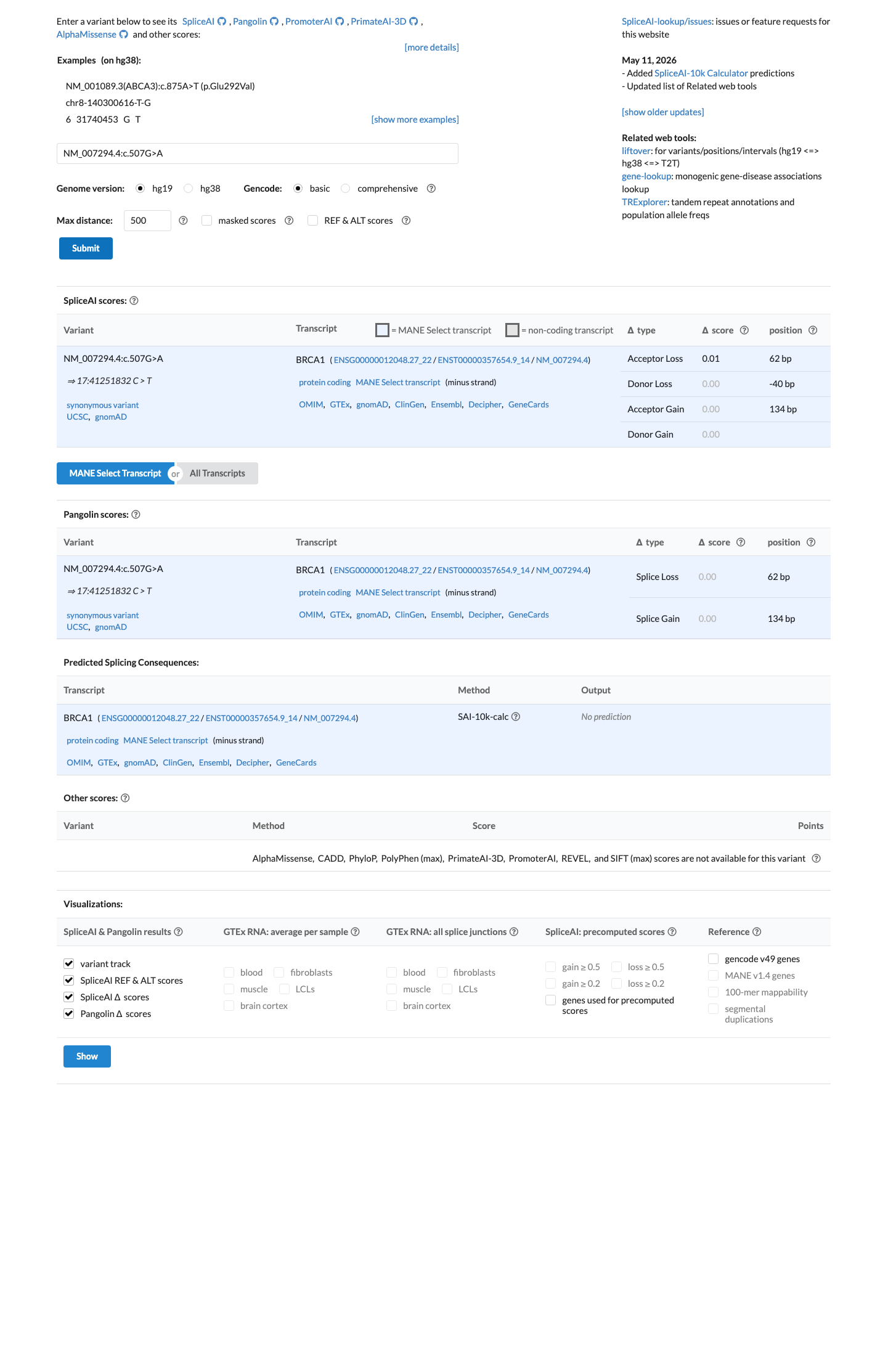
SpliceAI predicts no significant splice impact for this variant (max delta score = 0.01). REVEL score = 0.014.
Functional
Unknown Oncogenic Effect
OncoKB identified curated literature and non-variant-specific oncogenicity context for review; listed oncogenicity label: Unknown Oncogenic Effect.

COSMIC
Cancer hotspots
Somatic evidence
Not in COSMIC / hotspots
COSMIC
This variant does not lie in a statistically significant hotspot. This variant has not previously been reported in somatic cancers (COSMIC).
Hotspots
This variant does not lie in a statistically significant hotspot.
Sources & reference links
Triaged references · 9 PMIDs not cited in assessment
23918944 ↗
Tamoxifen and risk of contralateral breast cancer for BRCA1 and BRCA2 mutation carriers.
CLINVAR
25741868 ↗
Standards and guidelines for the interpretation of sequence variants: a joint consensus recommendation of the American College of Medical Genetics and Genomics and the Association for Molecular Pathology.
CLINVAR
26467025 ↗
A Standardized DNA Variant Scoring System for Pathogenicity Assessments in Mendelian Disorders.
CLINVAR
12692171 ↗
American Society of Clinical Oncology policy statement update: genetic testing for cancer susceptibility.
CLINVAR
15604628 ↗
Genetic cancer risk assessment and counseling: recommendations of the national society of genetic counselors.
CLINVAR
17392385 ↗
American Cancer Society guidelines for breast screening with MRI as an adjunct to mammography.
CLINVAR
17508274 ↗
Risk assessment and genetic counseling for hereditary breast and ovarian cancer: recommendations of the National Society of Genetic Counselors.
CLINVAR
28492532 ↗
Sherloc: a comprehensive refinement of the ACMG-AMP variant classification criteria.
CLINVAR