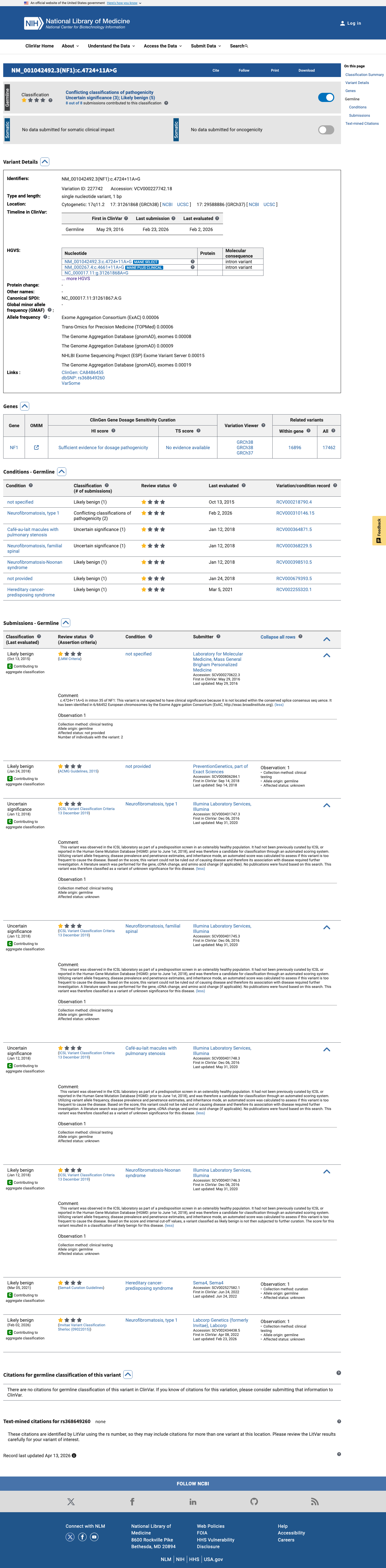
NM_000267.3:c.4661+11A>G is an intronic variant in NF1 (intron 34, +11 position) that has been observed in population databases at low frequency (gnomAD v2.1: 22/282,462 alleles, AF=0.0078%; v4.1: 281/1,612,590 alleles, AF=0.0174%).1 Computational splicing prediction (SpliceAI, max delta = 0.10) indicates no significant impact on mRNA splicing.2 A minigene splicing assay (Wimmer et al. 2007, PMID:17295913) demonstrated normal splicing of this variant with no exon skipping or cryptic splice site activation, providing functional evidence against a deleterious splicing effect (BS3_Supporting). Multiple clinical laboratories in ClinVar classify this variant as Likely benign (4 of 7 usable submissions), with no pathogenic classifications reported (BP6_Supporting).3 No pathogenic criteria are met. PVS1 is not applicable as this non-canonical intronic variant does not produce a null allele. PM2 is not met as the variant is present above absence thresholds. PS4 is not met due to population frequency inconsistent with a rare fully penetrant disorder. PS3 is not met as the only functional study shows normal splicing.4 Based on the available evidence (BS3_Supporting, BP4_Supporting, BP6_Supporting), this variant meets criteria for Likely benign classification. Note: BS3 is from a single minigene assay requiring verification; BP4 is from SpliceAI computational prediction; BP6 is from ClinVar clinical laboratory consensus without expert panel review.5
NF1
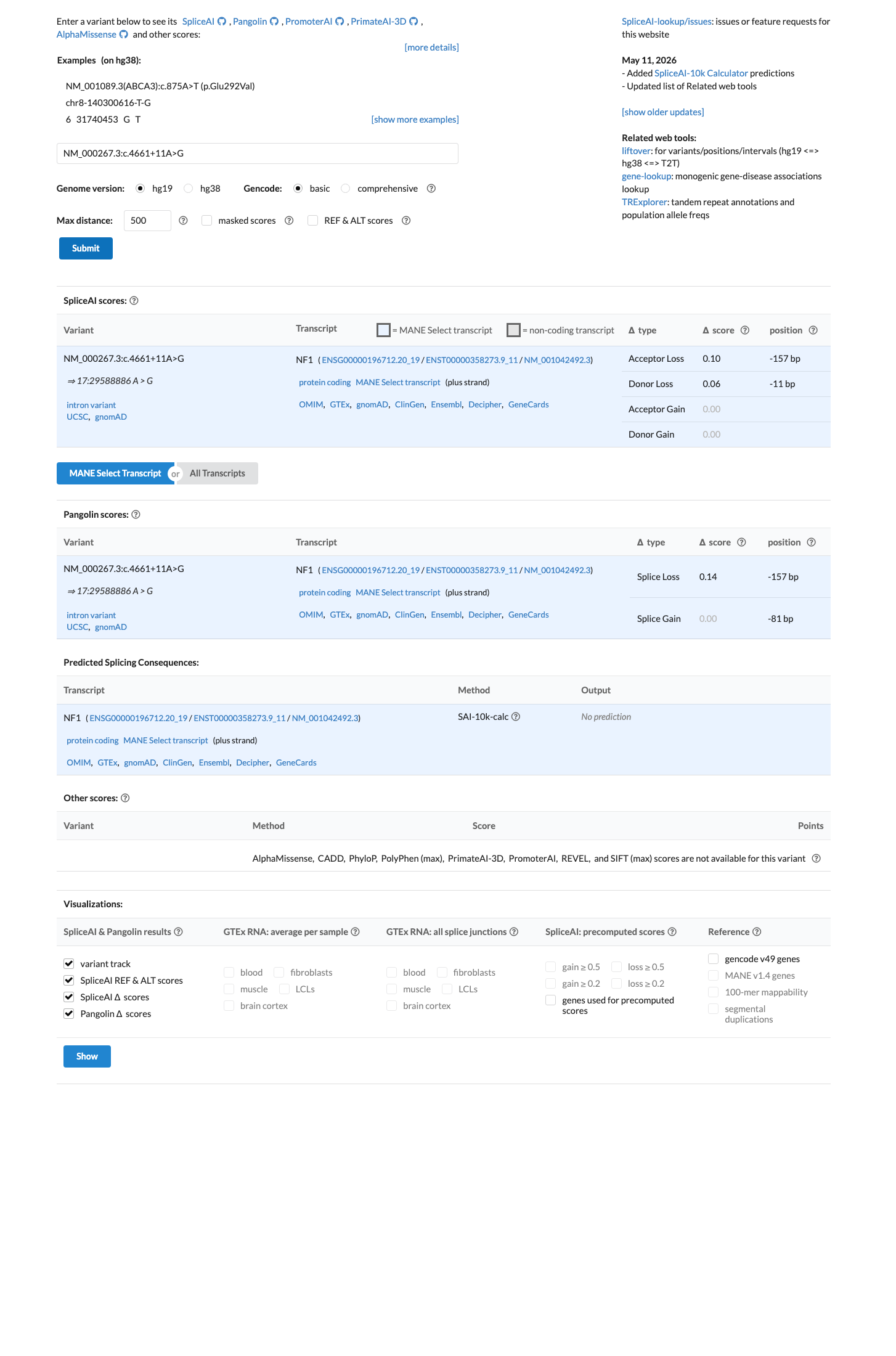
Final classification
Likely Benign
NF1 c.4661+11A>G · p.?
NF1
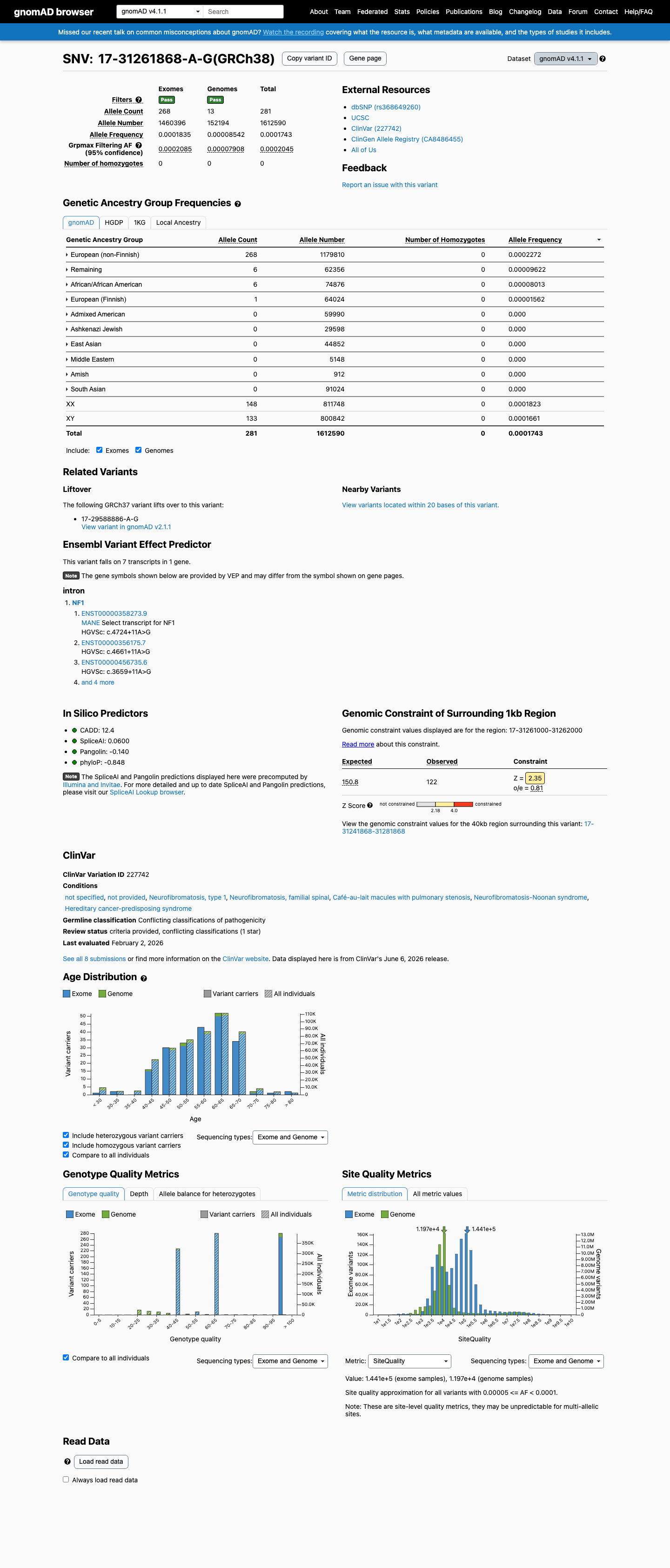
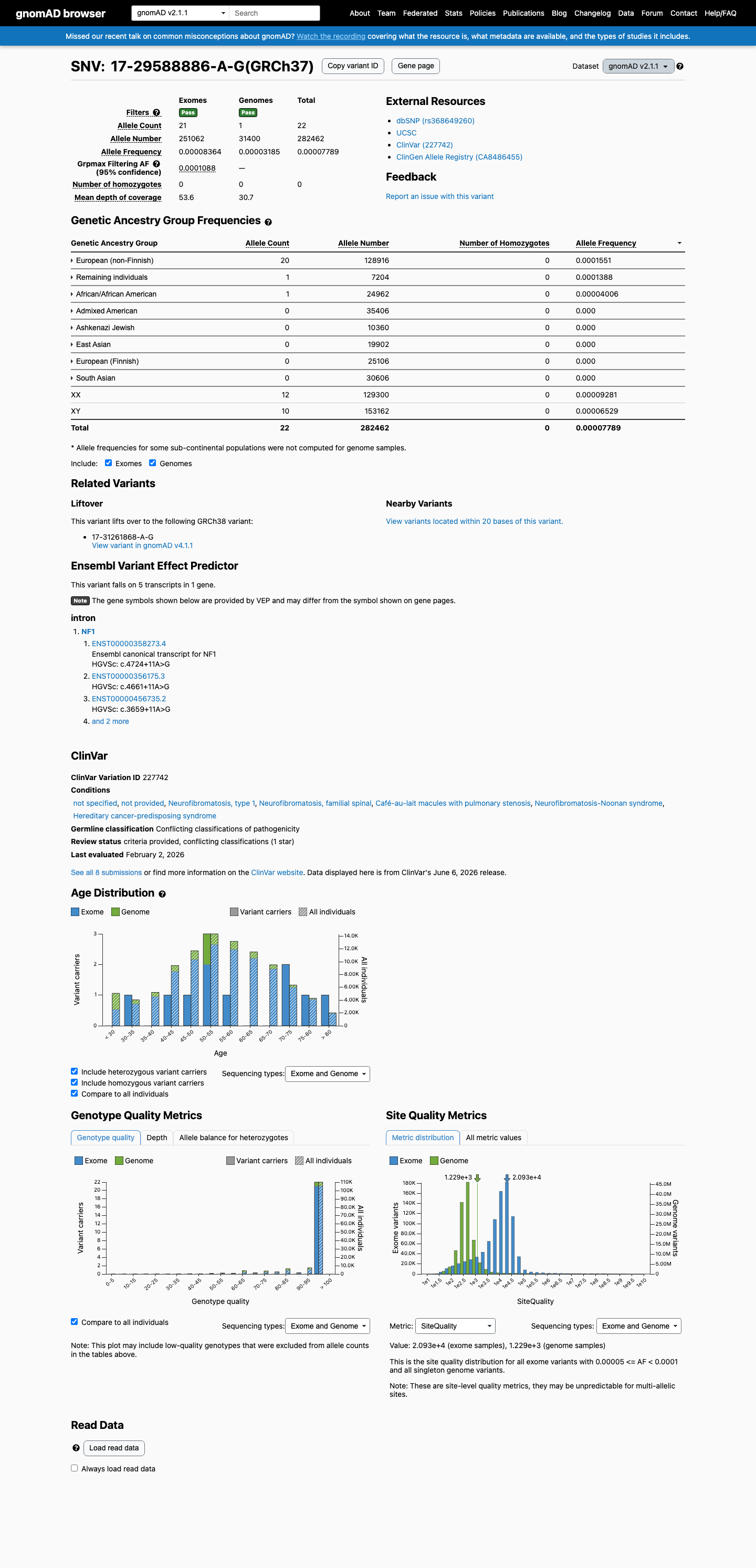
NM_000267.3:c.4661+11A>G is an intronic variant in NF1 (intron 34, +11 position) that has been observed in population databases at low frequency (gnomAD v2.1: 22/282,462 alleles, AF=0.0078%; v4.1: 281/1,612,590 alleles, AF=0.0174%).
Neurofibromatosis and Schwannomatosis Specification v1.0.0 lacked a usable explicit final combination framework, so generic ACMG/AMP 2015 final-combination rules were applied as fallback; applied criteria: BS3 supporting benign, BP4 supporting benign, BP6 supporting benign; combination = 3 supporting benign, which maps to Likely Benign.
Classification rationale
BS3BP4BP6
Likely Benign
NF1 c.4661+11A>G
BS3 + BP4 + BP6
→
Likely Benign
4
gnomad_v2 ↗gnomad_v4 ↗pvs1_variant_assessment
Gene diagram
· NM_000267.3 · variants mapped to exon structure
NF1
NM_000267.3
Fetching transcript structure from UCSC…
Applied criteria · 3 applied · 16 assessed
Applied · 3
Strength
Supporting
Moderate
Strong
Very strong
✓
BS3
supporting
review
Benign
Wimmer et al. (2007) performed a minigene splicing assay demonstrating normal splicing of c.4661+11A>G with no exon skipping or cryptic splice site activation. This well-established functional assay provides evidence that the variant does not impair mRNA splicing, supporting a benign effect. Note: this finding was identified through exploratory analysis and should be verified by reviewing the full text of PMID:17295913.
Minigene splicing assay demonstrated normal splicing (Wimmer et al. 2007PMID:17295913)No aberrant splicing or cryptic splice site activation detected
✓
BP4
supporting
Benign
SpliceAI predicts no significant splice impact (max delta score = 0.10). REVEL and BayesDel are not applicable for this intronic variant. The available computational evidence does not support a deleterious splicing effect.
SpliceAI max delta score = 0.10 (below commonly applied thresholds for splice-altering prediction)
✓
BP6
supporting
Benign
Multiple clinical diagnostic laboratories (4 of 7 usable submissions) classify this variant as Likely benign in ClinVar. The majority consensus among clinical testing laboratories provides reputable source evidence supporting a benign interpretation.
ClinVar: 4 Likely benign classifications from clinical laboratories3 Uncertain significance classificationsNo pathogenic classifications
Assessed · not applied
Pathogenic
PS2
No confirmed de novo occurrence with maternity and paternity testing has been reported in the literature for this variant.
PS3
The only functional study identified (Wimmer et al.
PS4
Although LOVD entries report multiple probands with NF1 carrying this variant, the variant is also observed in population databases at frequencies inconsistent with a fully penetrant rare disease allele (gnomAD v2.1: 22/282,462; v4.1: 281/1,612,590).
PM1
This intronic +11 position in intron 34 is not located in a well-established mutational hotspot or critical functional domain of NF1.
PM2
The variant is present in gnomAD at an allele frequency of 0.0078% (v2.1, 22/282,462 alleles) to 0.0174% (v4.1, 281/1,612,590 alleles), which exceeds the PM2 absence threshold (<0.1%) for a rare disease variant.
PM6
Exploratory search identified LOVD entries suggesting at least one apparently de novo occurrence without confirmed parentage.
PP1
Exploratory search identified LOVD entries suggesting co-segregation in two small families.
PP3
SpliceAI predicts no significant splice impact (max delta score = 0.10).
PP4
No patient-specific phenotypic data were provided with this case.
PP5
No reputable source has recently reported this variant as pathogenic.
Benign
BA1
The maximum allele frequency in gnomAD is 0.0227% (v4.1 European non-Finnish), which is well below the BA1 threshold of >1%.
BS1
The maximum allele frequency in gnomAD is 0.0227% (v4.1 European non-Finnish), which is below the BS1 threshold of >0.3%.
BS2
While the variant is observed in gnomAD at frequencies that suggest some carriers may be healthy adults (281 alleles in v4.1, with NF1 being nearly 100% penetrant by early childhood), gnomAD does not provide health status confirmation of carriers.
BS4
Exploratory search identified a ClinVar submission (reportedly variation 428109) suggesting inheritance from an unaffected parent.
BP2
No evidence of this variant occurring in trans with a known pathogenic NF1 variant has been reported.
BP5
No observation of this variant in a case where an alternative molecular basis for disease has been identified.
N/A · 7
PVS1 · PS1 · PM5 · PP2 · BP1 · BP3 · BP7
Research & evidence
Population frequency · supports benign
gnomAD v4.1
gnomAD v2.1
v4.1
This variant is present in gnomAD v4.1 (AF= 0.000174254; MAF= 0.01743%, 281/1612590 alleles, homozygotes = 0) and has highest observed frequency in the European (non-Finnish) population (AF= 0.000227155; MAF= 0.02272%, 268/1179810 alleles, homozygotes = 0); grpmax FAF= 0.00020451.
v2.1
This variant is present in gnomAD v2.1 (AF= 7.78866e-05; MAF= 0.00779%, 22/282462 alleles, homozygotes = 0) and has highest observed frequency in the European (non-Finnish) population (AF= 0.00015514; MAF= 0.01551%, 20/128916 alleles, homozygotes = 0); grpmax FAF= 0.00010881.
🇨🇦 CA
This variant is absent from gnomAD-Canada.
Allele frequency by ancestry
three datasets · side by side
gnomAD v4.1
0.017%
· 281 / 1,612,590
0 hom · FAF 0.02%
0 hom · FAF 0.02%
European (non-Finnish) 268 / 1,179,810 |
0.023% |
Remaining individuals 6 / 62,356 |
0.0096% |
African/African American 6 / 74,876 |
0.008% |
European (Finnish) 1 / 64,024 |
0.0016% |
+ 6 not observed (Admixed American, Amish, East Asian, Middle Eastern, South Asian, Ashkenazi Jewish)
gnomAD v2.1
0.0078%
· 22 / 282,462
0 hom · FAF 0.011%
0 hom · FAF 0.011%
European (non-Finnish) 20 / 128,916 |
0.016% |
Remaining individuals 1 / 7,204 |
0.014% |
African/African American 1 / 24,962 |
0.004% |
+ 5 not observed (Admixed American, Ashkenazi Jewish, East Asian, European (Finnish), South Asian)
gnomAD Canada 🇨🇦
Absent
· 0 / ?
0 hom
0 hom
Not observed in any ancestry group.
In silico
SpliceAI predicts no significant splice impact for this variant (max delta score = 0.10).
Functional
No data
No calibrated functional assay or RNA evidence was identified for this variant.

COSMIC
Somatic evidence
COSMIC
This variant has not previously been reported in somatic cancers (COSMIC).
Hotspots
This variant does not lie in a statistically significant cancer hotspot.
Literature · how each cited paper was used
1papers cited
Each card is an audit: what was searched, what was found, whether it names the variant, which criteria it fed, and why. 12 further PMIDs triaged but not cited — see Sources & References.
PMID 17295913
Found
2007 PMID:17295913) No aberrant splicing or cryptic splice site activation detected
Applied to
→BS3 supports · met
Sources & reference links
Triaged references · 12 PMIDs not cited in assessment
24033266 ↗
A systematic approach to assessing the clinical significance of genetic variants.
CLINVAR
25741868 ↗
Standards and guidelines for the interpretation of sequence variants: a joint consensus recommendation of the American College of Medical Genetics and Genomics and the Association for Molecular Pathology.
CLINVAR
15604628 ↗
Genetic cancer risk assessment and counseling: recommendations of the national society of genetic counselors.
CLINVAR
17636453 ↗
Neurofibromatosis type 1 in genetic counseling practice: recommendations of the National Society of Genetic Counselors.
CLINVAR
20065170 ↗
American Society of Clinical Oncology policy statement update: genetic and genomic testing for cancer susceptibility.
CLINVAR
20664475 ↗
The North American Neuroendocrine Tumor Society consensus guideline for the diagnosis and management of neuroendocrine tumors: pheochromocytoma, paraganglioma, and medullary thyroid cancer.
CLINVAR
24893135 ↗
Pheochromocytoma and paraganglioma: an endocrine society clinical practice guideline.
CLINVAR
26140447 ↗
Points to Consider: Ethical, Legal, and Psychosocial Implications of Genetic Testing in Children and Adolescents.
CLINVAR
28492532 ↗
Sherloc: a comprehensive refinement of the ACMG-AMP variant classification criteria.
CLINVAR
33939658 ↗
The North American Neuroendocrine Tumor Society Consensus Guidelines for Surveillance and Management of Metastatic and/or Unresectable Pheochromocytoma and Paraganglioma.
CLINVAR