NM_000368.5:c.1438+6G>A is present in gnomAD at very low allele frequency (0.010% in v2.1, 0.015% in v4.1; 28–243 alleles, no homozygotes), meeting PM2 at supporting strength.1 The variant is reported in ClinVar (ID 48782) with 10 of 15 clinical laboratory submissions classifying as Benign or Likely Benign, meeting BP6 at supporting benign strength. No submission classifies as Pathogenic.2 SpliceAI predicts no significant splicing impact (max delta score 0.10). No other computational or functional evidence supports or refutes a deleterious effect.3 PS2 (de novo), PS3 (functional), PS4 (case-control), PM6 (assumed de novo), PP1 (cosegregation), PP4 (patient phenotype), BS2 (healthy adults), BS3 (benign functional), BS4 (lack of segregation), BP2 (in trans/cis), and BP5 (alternate molecular basis) could not be assessed due to absence of variant-specific clinical or functional data. PVS1 is not met: the variant is at the +6 intronic position outside canonical ±1,2 splice sites, and SpliceAI does not predict a splice alteration. The variant does not qualify as a predicted null variant under ClinGen SVI PVS1 recommendations.4 Using the generic ACMG/AMP 2015 combination rules (PMID:25741868), the variant has one supporting pathogenic criterion (PM2) and one supporting benign criterion (BP6). The net point score is 0, resulting in a classification of Variant of Uncertain Significance (VUS). This is consistent with the conflicting ClinVar aggregate classification.5
TSC1
Final classification
VUS
TSC1 c.1438+6G>A · p.?
TSC1
NM_000368.5:c.1438+6G>A is present in gnomAD at very low allele frequency (0.010% in v2.1, 0.015% in v4.1; 28–243 alleles, no homozygotes), meeting PM2 at supporting strength.
gene-specific framework lacked a usable explicit final combination framework, so generic ACMG/AMP 2015 final-combination rules were applied as fallback; applied criteria: PM2 supporting, BP6 supporting benign; combination = 1 supporting + 1 supporting benign, which maps to VUS.
Classification rationale
PM2
BP6
VUS
TSC1 c.1438+6G>A
PM2 + BP6
→
VUS
4
pvs1_generic_framework ↗pvs1_variant_assessmentspliceai ↗
Gene diagram
· NM_000368.5 · variants mapped to exon structure
TSC1
NM_000368.5
Fetching transcript structure from UCSC…
Applied criteria · 2 applied · 18 assessed
Applied · 2
Strength
Supporting
Moderate
Strong
Very strong
✓
PM2
supporting
Pathogenic
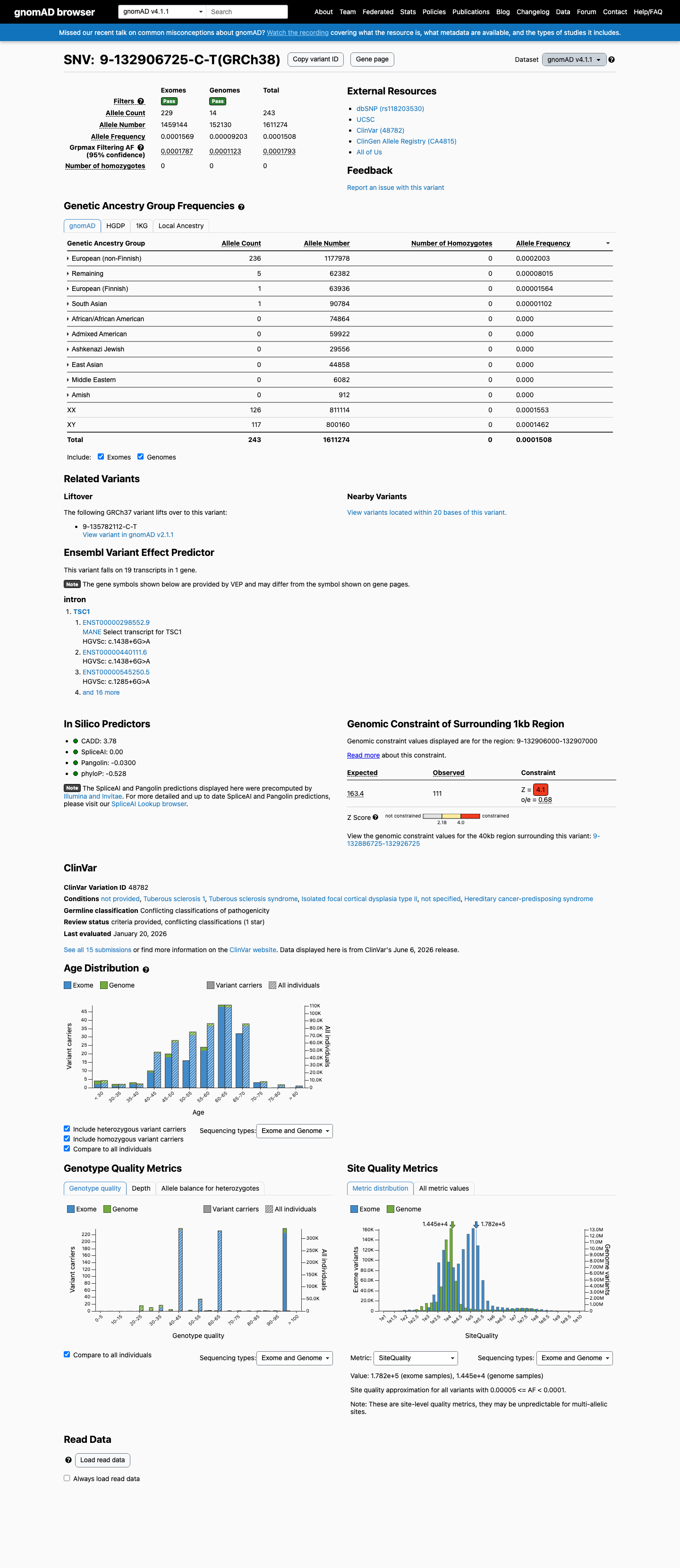
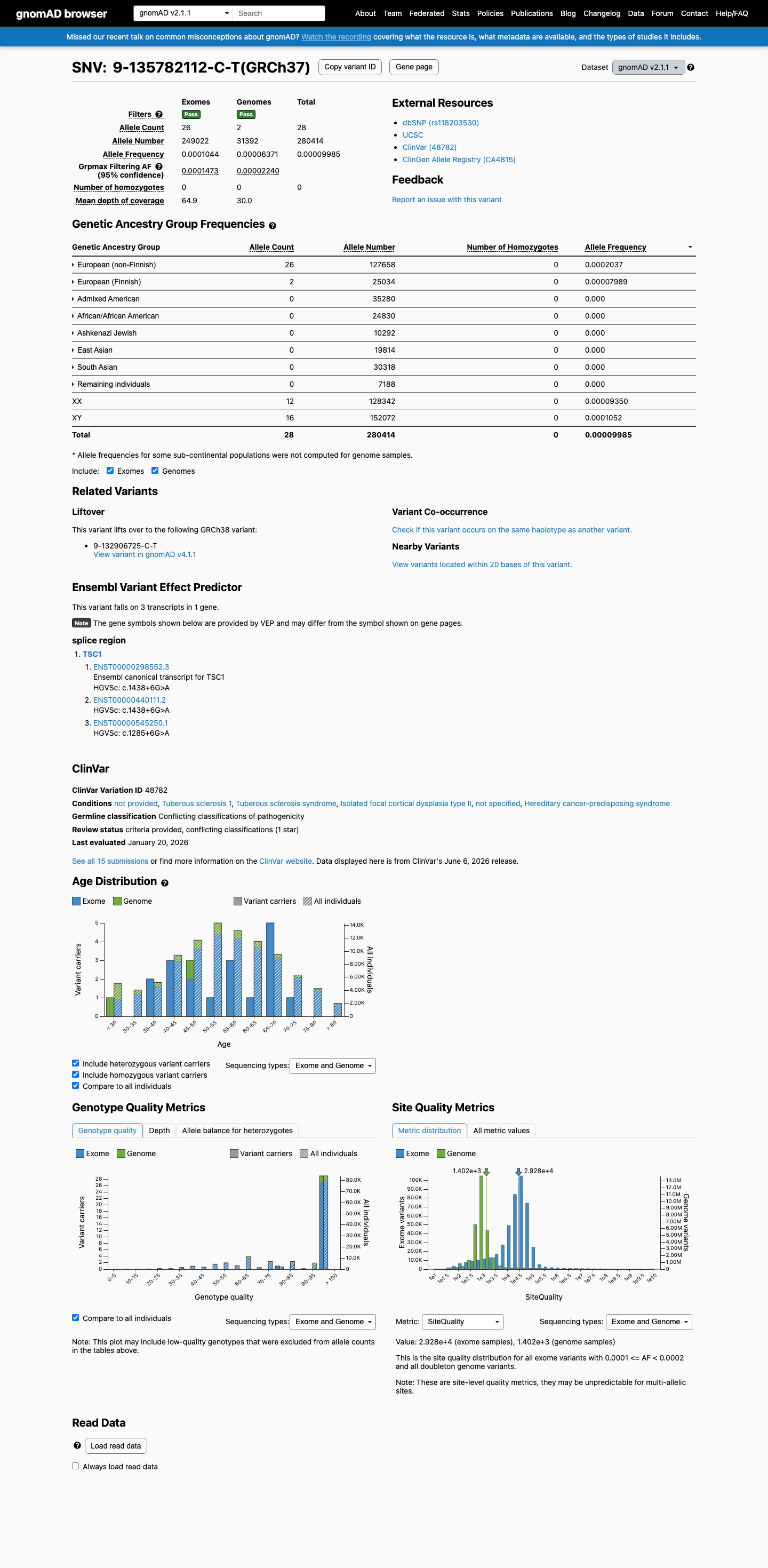
NM_000368.5:c.1438+6G>A is present in gnomAD at very low allele frequency: 0.00999% (28/280,414 alleles, no homozygotes) in v2.1 and 0.01508% (243/1,611,274 alleles, no homozygotes) in v4.1, with grpmax filtering AF of 0.000147 (v2.1) and 0.000179 (v4.1). The allele frequency is well below the 0.1% threshold for PM2 in a dominant disorder gene.
gnomAD v2.1: 28/280414 alleles (AF=0.010%)0 homozygotes
✓
BP6
supporting
Benign
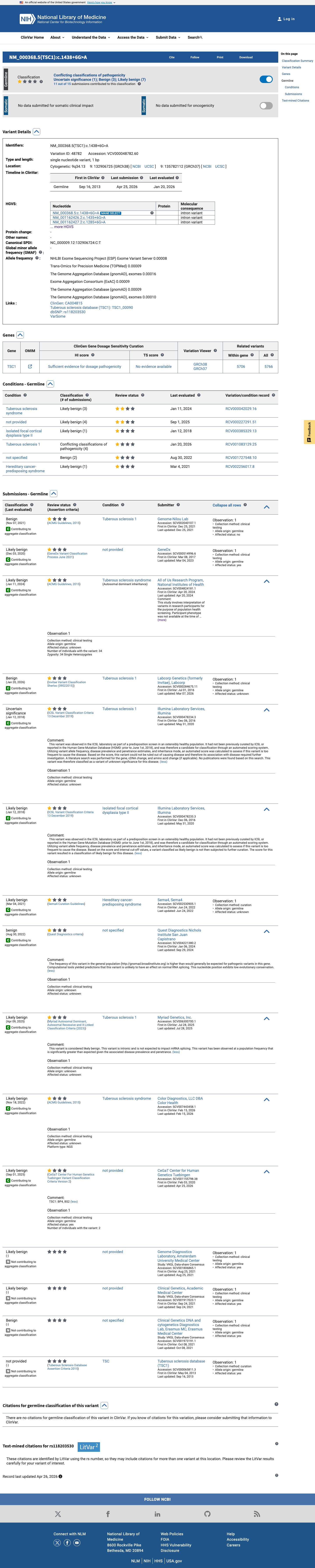
BP6 applies when a reputable source reports the variant as benign with supporting evidence not independently available. ClinVar aggregate classification (ID 48782) for NM_000368.5:c.1438+6G>A is conflicting but predominantly benign: 10 of 15 clinical laboratory submissions classify the variant as Benign (3 submissions), Likely benign (7 submissions), or Likely Benign (1 submission), with only 1 Uncertain significance submission. The weight of clinical laboratory consensus supports application of BP6 at supporting benign strength. No expert panel has reviewed this variant.
ClinVar ID 48782: 10/15 submissions Benign or Likely BenignMultiple clinical laboratories: Labcorp/Invitae (Benign)GeneDx (Likely benign)
Assessed · not applied
Pathogenic
PVS1
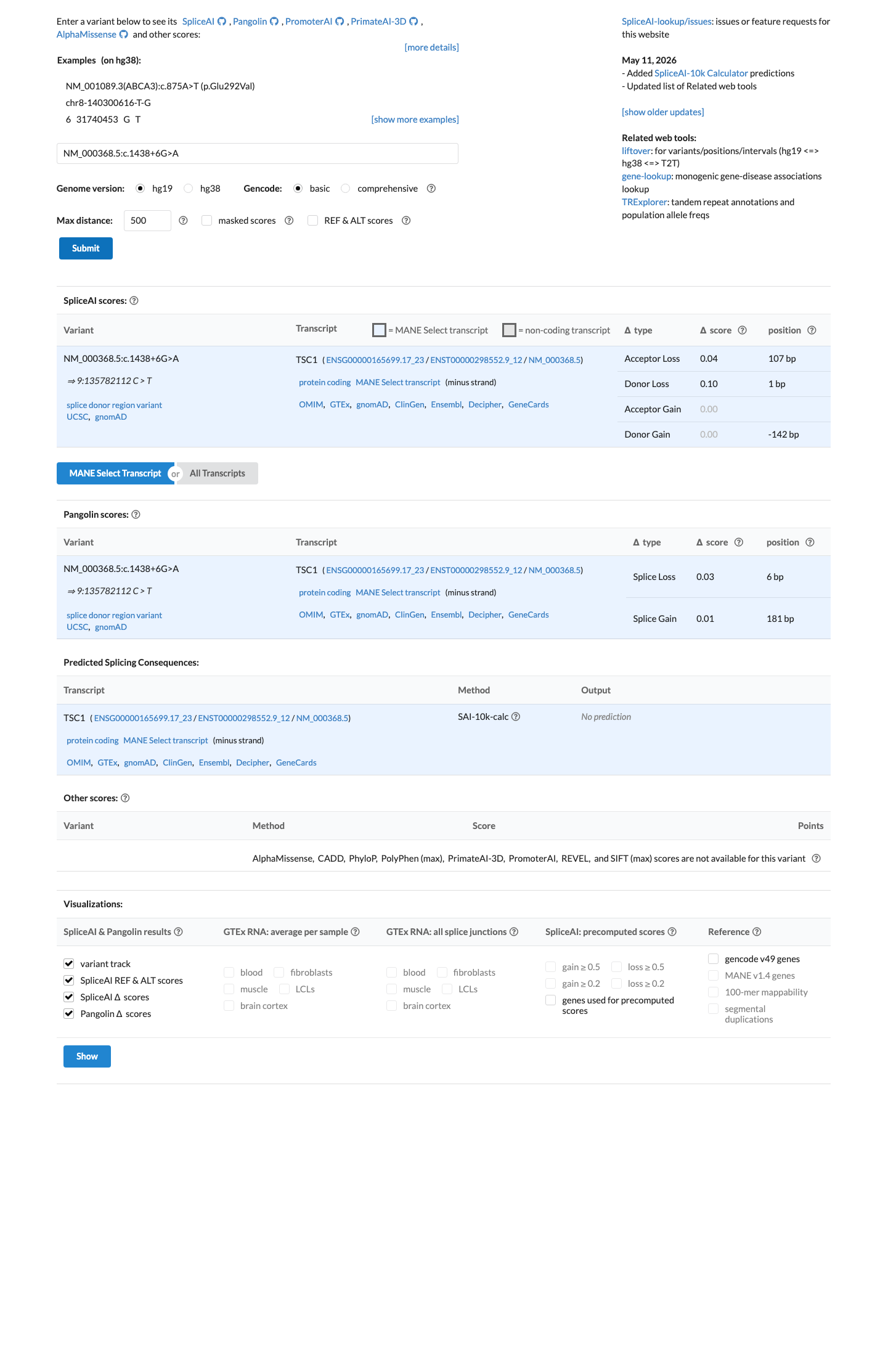
NM_000368.5:c.1438+6G>A is an intronic variant at the donor splice site +6 position, outside the canonical ±1,2 splice consensus.
PS2
PS2 requires a confirmed de novo occurrence with both parental relationships confirmed in a patient with the disease and no family history.
PS3
PS3 requires well-established in vitro or in vivo functional studies demonstrating a damaging effect.
PS4
PS4 requires statistically higher prevalence of the variant in affected individuals versus controls.
PM1
PM1 applies to variants located in a mutational hotspot or critical functional domain.
PM6
PM6 requires an assumed de novo occurrence without confirmation of paternity and maternity.
PP1
PP1 requires cosegregation of the variant with disease in multiple affected family members.
PP3
PP3 requires multiple lines of computational evidence supporting a deleterious effect.
PP4
PP4 requires a patient's phenotype or family history to be highly specific for a disease with a single genetic etiology.
PP5
PP5 requires a reputable source to report the variant as pathogenic with supporting evidence.
Benign
BA1
BA1 requires an allele frequency >1% in population databases.
BS1
BS1 requires an allele frequency >0.3% in population databases for a dominant disorder.
BS2
BS2 requires observation of the variant in a healthy adult individual with full penetrance expected at an early age.
BS3
BS3 requires well-established in vitro or in vivo functional studies showing no damaging effect.
BS4
BS4 requires lack of segregation of the variant with disease in affected family members.
BP2
BP2 requires observation of the variant in trans with a known pathogenic variant in a fully penetrant dominant disorder, or in cis with a pathogenic variant.
BP4
BP4 requires multiple lines of computational evidence suggesting no impact on gene or gene product.
BP5
BP5 requires identification of an alternate molecular basis for disease in a case where the variant was observed.
N/A · 5
PS1 · PM5 · PP2 · BP1 · BP7
Research & evidence
Population frequency
gnomAD v4.1
gnomAD v2.1
v4.1
This variant is present in gnomAD v4.1 (AF= 0.000150812; MAF= 0.01508%, 243/1611274 alleles, homozygotes = 0) and has highest observed frequency in the European (non-Finnish) population (AF= 0.000200343; MAF= 0.02003%, 236/1177978 alleles, homozygotes = 0); grpmax FAF= 0.00017932.
v2.1
This variant is present in gnomAD v2.1 (AF= 9.98524e-05; MAF= 0.00999%, 28/280414 alleles, homozygotes = 0) and has highest observed frequency in the European (non-Finnish) population (AF= 0.000203669; MAF= 0.02037%, 26/127658 alleles, homozygotes = 0); grpmax FAF= 0.00014731.
🇨🇦 CA
This variant is absent from gnomAD-Canada.
Allele frequency by ancestry
three datasets · side by side
gnomAD v4.1
0.015%
· 243 / 1,611,274
0 hom · FAF 0.018%
0 hom · FAF 0.018%
European (non-Finnish) 236 / 1,177,978 |
0.02% |
Remaining individuals 5 / 62,382 |
0.008% |
European (Finnish) 1 / 63,936 |
0.0016% |
South Asian 1 / 90,784 |
0.0011% |
+ 6 not observed (Admixed American, Amish, East Asian, Middle Eastern, Ashkenazi Jewish, African/African American)
gnomAD v2.1
0.01%
· 28 / 280,414
0 hom · FAF 0.015%
0 hom · FAF 0.015%
European (non-Finnish) 26 / 127,658 |
0.02% |
European (Finnish) 2 / 25,034 |
0.008% |
+ 6 not observed (African/African American, Admixed American, Ashkenazi Jewish, East Asian, Remaining individuals, South Asian)
gnomAD Canada 🇨🇦
Absent
· 0 / ?
0 hom
0 hom
Not observed in any ancestry group.
ClinVar
This variant has been reported in ClinVar as Likely benign (7 clinical laboratories) and as Benign (3 clinical laboratories) and as Likely Benign (1 clinical laboratory) and as Uncertain significance (1 clinical laboratory) and as benign (1 clinical laboratory). (ClinVarID = 48782)
In silico
SpliceAI predicts no significant splice impact for this variant (max delta score = 0.10).
Functional
No data
No calibrated functional assay or RNA evidence was identified for this variant.

COSMIC
Somatic evidence
COSMIC
This variant has not previously been reported in somatic cancers (COSMIC).
Hotspots
This variant does not lie in a statistically significant cancer hotspot.
Sources & reference links
Triaged references · 9 PMIDs not cited in assessment
25741868 ↗
Standards and guidelines for the interpretation of sequence variants: a joint consensus recommendation of the American College of Medical Genetics and Genomics and the Association for Molecular Pathology.
CLINVAR
26467025 ↗
A Standardized DNA Variant Scoring System for Pathogenicity Assessments in Mendelian Disorders.
CLINVAR
23519317 ↗
Clinical genetics evaluation in identifying the etiology of autism spectrum disorders: 2013 guideline revisions.
CLINVAR
23788249 ↗
ACMG recommendations for reporting of incidental findings in clinical exome and genome sequencing.
CLINVAR
25356965 ↗
ACMG policy statement: updated recommendations regarding analysis and reporting of secondary findings in clinical genome-scale sequencing.
CLINVAR
25394175 ↗
A practice guideline from the American College of Medical Genetics and Genomics and the National Society of Genetic Counselors: referral indications for cancer predisposition assessment.
CLINVAR
27854360 ↗
Recommendations for reporting of secondary findings in clinical exome and genome sequencing, 2016 update (ACMG SF v2.0): a policy statement of the American College of Medical Genetics and Genomics.
CLINVAR
28492532 ↗
Sherloc: a comprehensive refinement of the ACMG-AMP variant classification criteria.
CLINVAR