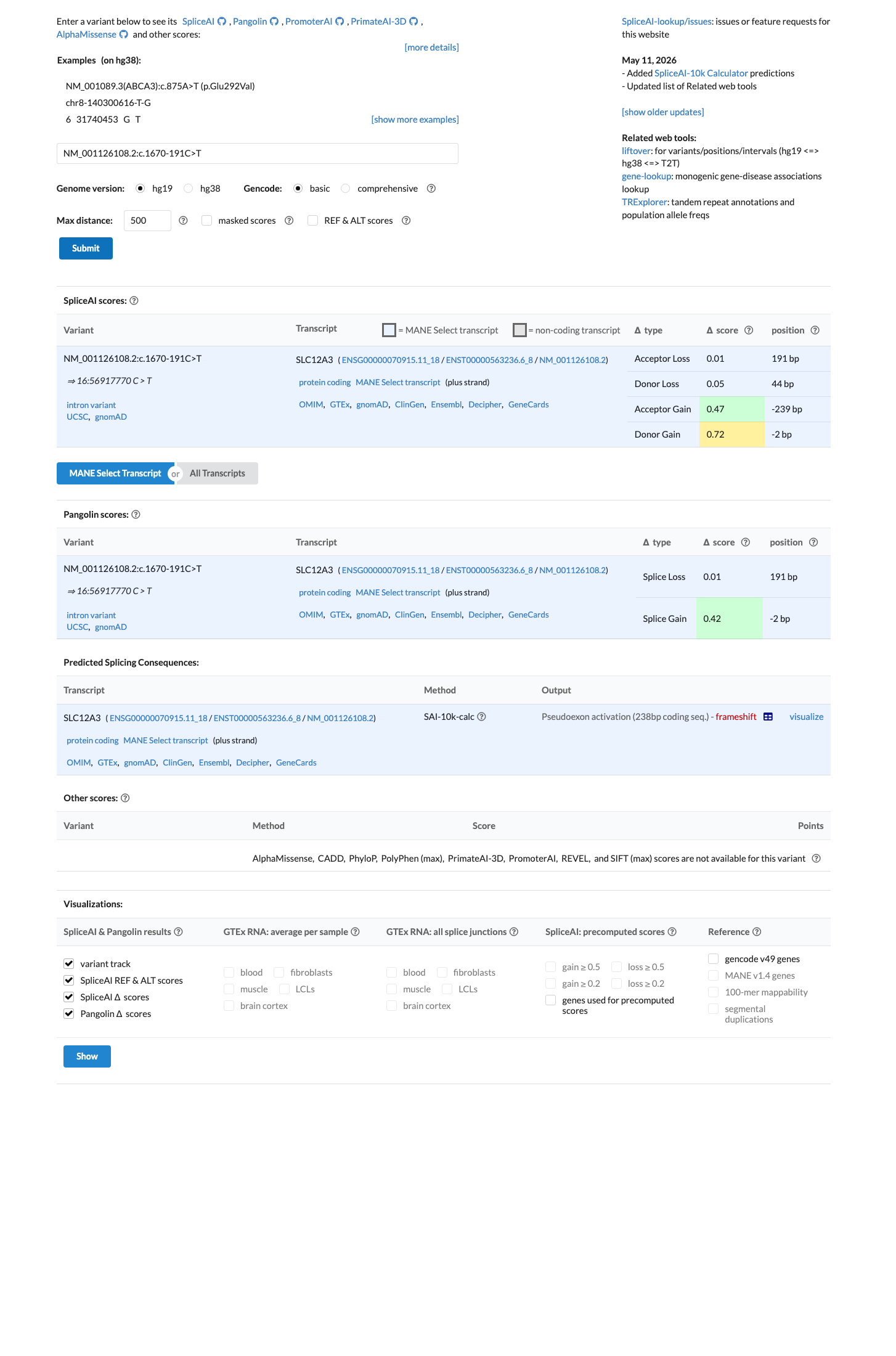
c.1670-191C>T is a deep intronic substitution in intron 13 of SLC12A3 that creates a novel donor splice site, leading to 238-bp cryptic exon inclusion and a premature termination codon, as demonstrated by RT-PCR from patient leukocytes and urine sediments.1 RNA and immunohistochemistry analyses in 19 patients from 14 families confirmed cryptic exon inclusion and marked attenuation of NCC expression in the distal convoluted tubule, establishing the variant as a recurrent pathogenic deep intronic mutation in Gitelman syndrome.2 Independent midigene splice assays confirmed aberrant splicing with activation of a cryptic splice donor site, further validating the damaging molecular mechanism.3 The variant is extremely rare in population databases: gnomAD v2.1 allele frequency is 0.0032% (1/31,384 alleles) and gnomAD v4.1 allele frequency is 0.0013% (2/152,332 alleles), with no homozygotes observed.4 At least 27 unrelated probands with biochemically confirmed Gitelman syndrome have been reported to carry this variant across multiple independent studies, consistent with a substantial enrichment in affected individuals compared to the general population.5 SpliceAI in silico prediction supports a deleterious splicing effect with a maximum delta score of 0.72, consistent with the experimentally confirmed cryptic splice site activation.6 Gitelman syndrome is a well-characterized autosomal recessive salt-losing tubulopathy for which SLC12A3 is the established disease gene, and the patients' clinical phenotypes (hypokalemia, hypomagnesemia, metabolic alkalosis, hypocalciuria) are highly specific.7 Applying the generic ACMG/AMP 2015 combination rules: PS3 (strong), PS4 (moderate), PM2 (supporting), PP3 (supporting), and PP4 (supporting) yields a classification of Pathogenic (1 strong + 1 moderate + 3 supporting).8
SLC12A3
Final classification
Likely Pathogenic
SLC12A3 c.1670-191C>T · p.?
SLC12A3
c.1670-191C>T is a deep intronic substitution in intron 13 of SLC12A3 that creates a novel donor splice site, leading to 238-bp cryptic exon inclusion and a premature termination codon, as demonstrated by RT-PCR from patient leukocytes and urine sediments.
gene-specific framework lacked a usable explicit final combination framework, so generic ACMG/AMP 2015 final-combination rules were applied as fallback; applied criteria: PS3 strong, PS4 moderate, PM2 supporting, PP3 supporting, PP4 supporting; combination = 1 strong + 1 moderate + 3 supporting, which maps to Likely Pathogenic.
Classification rationale
PS3PS4PM2PP3PP4
Likely Pathogenic
SLC12A3 c.1670-191C>T
PS3 + PS4 + PM2 + PP3 + PP4
→
Likely Pathogenic
8
generic_acmg_combination_rules
Gene diagram
· NM_001126108.2 · variants mapped to exon structure
SLC12A3
NM_001126108.2
Fetching transcript structure from UCSC…
Applied criteria · 5 met · select any tile
Met
Not met
Not assessed
N/A
Strength
very strong
supporting
Pathogenic evidence
PVS
PS
PM
PP
Benign evidence
BA
BS
BP
—
—
—
Rationale
Select a criterion.
Sources
Evidence used
Gaps remaining
Rule
—
Research & evidence
Population frequency · supports pathogenic
gnomAD v4.1
gnomAD v2.1
v4.1
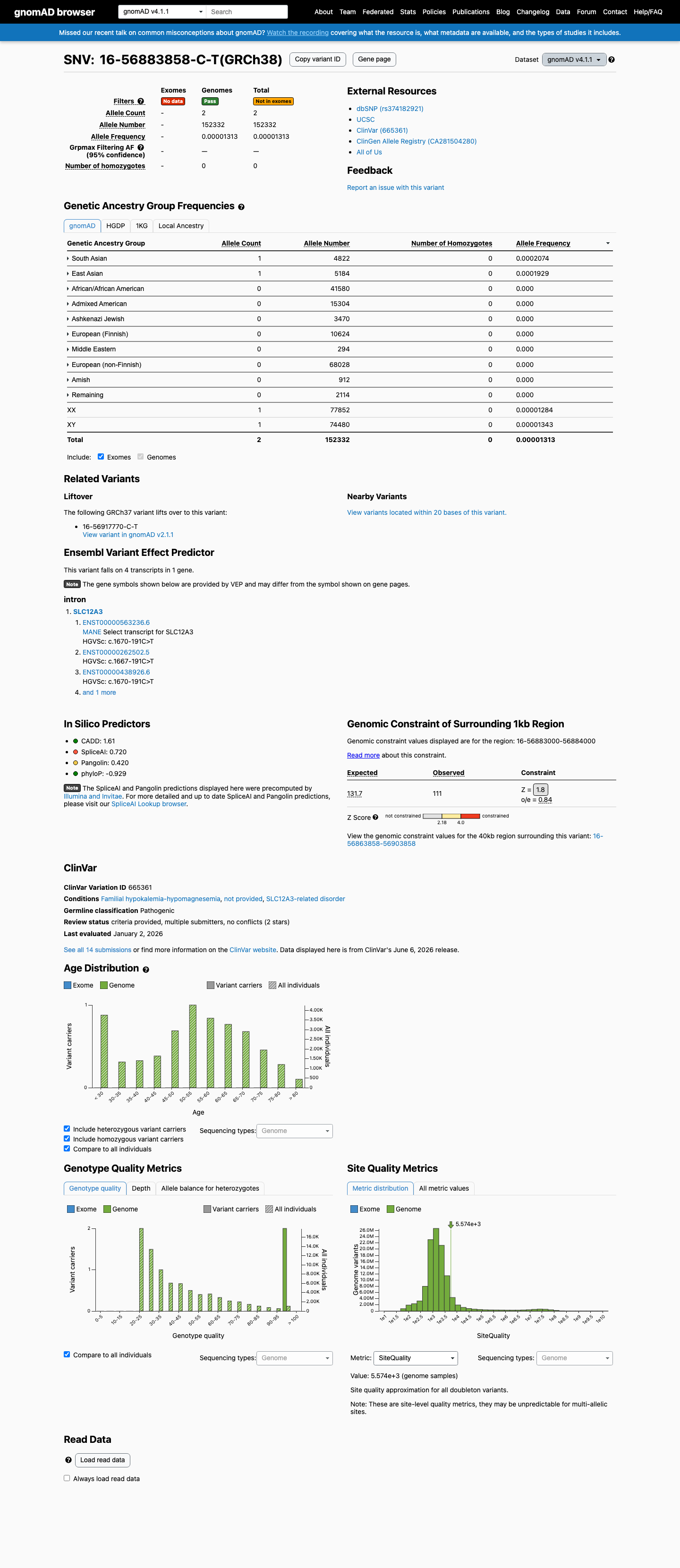
This variant is present in gnomAD v4.1 (AF= 1.31292e-05; MAF= 0.00131%, 2/152332 alleles, homozygotes = 0) and has highest observed frequency in the South Asian population (AF= 0.000207383; MAF= 0.02074%, 1/4822 alleles, homozygotes = 0).
v2.1
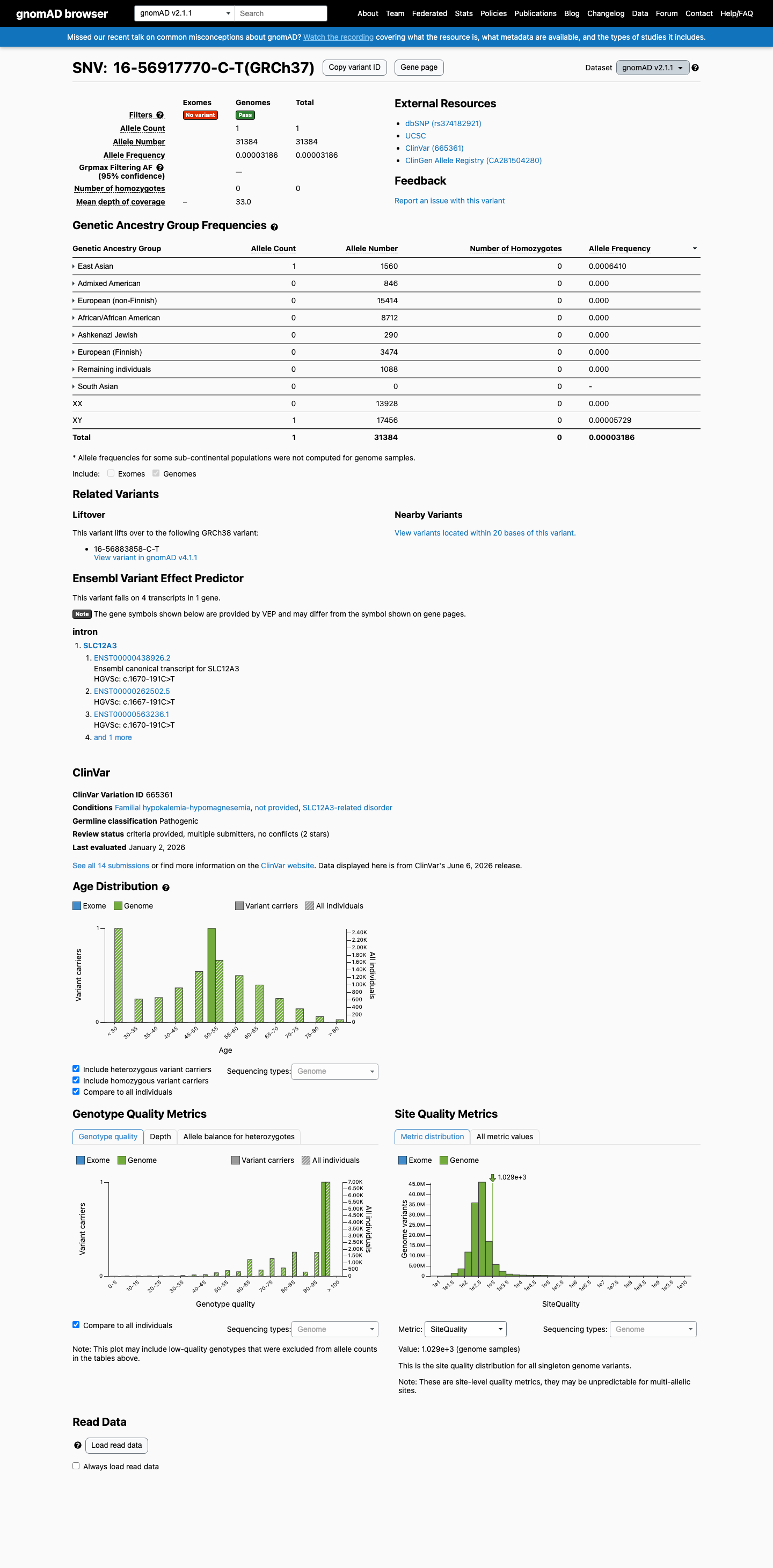
This variant is present in gnomAD v2.1 (AF= 3.18634e-05; MAF= 0.00319%, 1/31384 alleles, homozygotes = 0) and has highest observed frequency in the East Asian population (AF= 0.000641026; MAF= 0.06410%, 1/1560 alleles, homozygotes = 0).
🇨🇦 CA
This variant is present in gnomAD-Canada v1.0 (AF= 0.00016291951775822744, 3/18414 alleles, homozygotes = 0).
Allele frequency by ancestry
three datasets · side by side
gnomAD v4.1
0.0013%
· 2 / 152,332
0 hom
0 hom
South Asian 1 / 4,822 |
0.021% |
East Asian 1 / 5,184 |
0.019% |
+ 8 not observed (Remaining individuals, Admixed American, European (Finnish), Amish, Middle Eastern, Ashkenazi Jewish, African/African American, European (non-Finnish))
gnomAD v2.1
0.0032%
· 1 / 31,384
0 hom
0 hom
East Asian 1 / 1,560 |
0.064% |
+ 7 not observed (African/African American, Admixed American, Ashkenazi Jewish, European (Finnish), European (non-Finnish), Remaining individuals, South Asian)
gnomAD Canada 🇨🇦
0.016%
· 3 / 18,414
0 hom · FAF 0.027%
0 hom · FAF 0.027%
East Asian 2 / 1,336 |
0.15% |
European (non-Finnish) 1 / 11,738 |
0.0085% |
+ 7 not observed (African/African American, Latino/Admixed American, Ashkenazi Jewish, European (Finnish), Middle Eastern, Remaining individuals, South Asian)

ClinVar
This variant has been reported in ClinVar as Pathogenic (13 clinical laboratories). (ClinVarID = 665361)
In silico
SpliceAI predicts possible splice impact for this variant (max delta score = 0.72).
Functional
No data
No calibrated functional assay or RNA evidence was identified for this variant.

COSMIC
Somatic evidence
COSMIC
This variant has not previously been reported in somatic cancers (COSMIC).
Hotspots
This variant does not lie in a statistically significant cancer hotspot.
Literature · how each cited paper was used
9papers cited
Each card is an audit: what was searched, what was found, whether it names the variant, which criteria it fed, and why. 3 further PMIDs triaged but not cited — see Sources & References.
A deep intronic mutation in the SLC12A3 gene leads to Gitelman syndrome.
Searched
c.1670-191C>Tc.1670–191C→Tc.1670-1911670-191
Found
First report of c.1670-191C>T in a 12-year-old girl with Gitelman syndrome. RT-PCR from leukocytes and urine sediments demonstrated a 238-bp cryptic exon inclusion between exons 13 and 14 caused by a novel donor splice site, creating a premature stop codon. The patient was compound heterozygous with c.818_819insG in exon 6. The variant was absent from 200 control chromosomes.
Variant
✓ Names this variant — characterised directly
Applied to
→PS3 supports · met
→PS4 supports · met
Why
Discovery paper for this variant; provides foundational functional evidence for PS3 and clinical observation for PS4.
The genomic DNA analysis of intron 13 revealed a single-base substitution (c.1670–191C→T) that creates a new donor splice site within the intron resulting in the inclusion of a novel cryptic exon in mRNA.
Location Abstract; Results paragraphs 1-2; Figures 1C, 2, 4; Discussion paragraphs 1-2 · Context RT-PCR from patient blood leukocytes and urine sediment RNA; subcloning and Sanger sequencing; SLC12A3 transcript analysis (exons 13-15) · full text
Recurrent deep intronic mutations in the SLC12A3 gene responsible for Gitelman's syndrome.
Searched
c.1670-191C>Tc.1670–191C→Tc.1670−191C→T1670-191
Found
Identification of c.1670-191C>T as a recurrent deep intronic mutation in 19 Gitelman syndrome patients from 14 families, including 9 Taiwan aboriginal patients with homozygous mutations. RT-PCR confirmed 238-bp cryptic exon inclusion. Immunohistochemistry of renal tissue from a homozygous patient showed marked attenuation of NCC expression in the distal convoluted tubule. Haplotype analysis indicated the variant is a mutational hot spot rather than a founder effect.
Variant
✓ Names this variant — characterised directly
Applied to
→PS3 supports · met
→PS4 supports · met
Why
Largest patient series for this variant; provides strong functional evidence (PS3 strong) and substantial clinical observations (PS4 moderate).
We identified nine Taiwan aboriginal patients carrying c.1670–191C→T mutations in intron 13 and 10 nonaboriginal patients with c.2548+253C→T mutations in intron 21.
Location Abstract; Results (Identification of Deep Intronic Mutations, Functional Significance); Table 1; Table 3; Figures 2, 4 · Context RT-PCR from leukocyte RNA; immunohistochemistry of NCC in human renal biopsy tissue; haplotype analysis with microsatellite markers flanking SLC12A3 · full text
Successful application of genome sequencing in a diagnostic setting: 1007 index cases from a clinically heterogeneous cohort.
Searched
c.1670-191C>Tc.1670–191C>T1670-191
Found
Genome sequencing of 1007 index cases identified c.1670-191C>T in the homozygous state in one patient with Gitelman syndrome. The variant was listed among pathogenic/likely pathogenic variants detected in the diagnostic cohort.
Variant
✓ Names this variant — characterised directly
Applied to
→PS4 supports · met
Why
Provides an additional independent proband observation supporting PS4. The homozygous state is consistent with autosomal recessive Gitelman syndrome.
NM_000339.2 (SLC12A3):c.1670–191C>T NC_000016.9:g.56917770C>T Hom P Gitelman syndrome
Location Supplementary material (variant table); Results · Context Clinical genome sequencing diagnostic cohort (CENTOGENE) · full text
Long-Read Sequencing Identifies Novel Pathogenic Intronic Variants in Gitelman Syndrome.
Searched
c.1670-191C>Tc.1670-1911670-191
Found
Long-read sequencing study of Gitelman syndrome patients. Midigene splice assays of c.1670-191C>T confirmed aberrant splicing through activation of a cryptic splice donor site. The variant was identified in 7 patients and described as 'truly recurrent.' The c.1670-191 position was noted to have propensity to mutate to thymine, explaining recurrence.
Variant
✓ Names this variant — characterised directly
Applied to
→PS3 supports · met
→PS4 supports · met
Why
Independent replication of functional splicing defect using midigene assay; supports PS3 and PS4 with additional patient observations.
Midigene splice assays of the previously known c.1670-191C>T variant and intronic candidate variants demonstrated aberrant splicing.
Location Results (Midigene Splice Assays, Table 1); Discussion · Context Midigene splice assays in HEK293T cells; long-read sequencing (Pacific Biosciences) · full text
PMID PMID:19668106
Found
Structured finding pending for this record — see source link.
Applied to
→PS3 supports · met
PMID PMID:21051746
Found
Structured finding pending for this record — see source link.
Applied to
→PS3 supports · met
→PS4 supports · met
PMID PMID:21343949
Found
Structured finding pending for this record — see source link.
Applied to
→PP4 supports · met
PMID PMID:32860008
Found
Structured finding pending for this record — see source link.
Applied to
→PS4 supports · met
PMID PMID:36302598
Found
Structured finding pending for this record — see source link.
Applied to
→PS3 supports · met
→PS4 supports · met
Sources & reference links
Triaged references · 3 PMIDs not cited in assessment
25741868 ↗
Standards and guidelines for the interpretation of sequence variants: a joint consensus recommendation of the American College of Medical Genetics and Genomics and the Association for Molecular Pathology.
CLINVAR
28492532 ↗
Sherloc: a comprehensive refinement of the ACMG-AMP variant classification criteria.
CLINVAR