The BRAF c.736G>C (p.Ala246Pro) missense variant is absent from gnomAD population databases (PM2_Supporting).1 The variant lies within exon 6, a critical functional domain defined by the ClinGen RASopathy VCEP v2.3.0 (PM1_Moderate).2 The variant has been observed in multiple unrelated probands with cardio-facio-cutaneous syndrome, including the original CFC discovery cohort (Niihori et al. 2006), and is classified as Pathogenic by the ClinGen RASopathy VCEP in ClinVar with submissions from 9 clinical laboratories (PS4_Supporting).3 A de novo occurrence was reported in a CFC proband with both parents negative, though without molecular confirmation of parentage (PM6_Supporting).4 In silico predictions support a deleterious effect: REVEL score is 0.928, exceeding the VCEP threshold of 0.7 (PP3).5 BRAF exhibits a high gnomAD missense z-score (>3.09), indicating constraint against missense variation, and missense variants are a common disease mechanism for RASopathies (PP2).6 Functional studies by Wen et al. 2013 demonstrated that A246P increases Ras binding affinity relative to wild-type, consistent with a gain-of-function mechanism, though the assay is not in the VCEP-approved functional studies list (PS3 not assessed).7 Under the ClinGen RASopathy VCEP v2.3.0 combination rules (Rule15: 1 moderate + ≥4 supporting → Likely Pathogenic), the variant meets PM1 (moderate) plus PM2_Supporting, PM6_Supporting, PS4_Supporting, PP2, and PP3 (5 supporting criteria), resulting in a classification of Likely Pathogenic.8
BRAF
Final classification
Likely Pathogenic
BRAF c.736G>C · p.Ala246Pro
BRAF
The BRAF c.736G>C (p.Ala246Pro) missense variant is absent from gnomAD population databases (PM2_Supporting).
ClinGen RASopathy Expert Panel Specifications to the ACMG/AMP Variant Interpretation Guidelines for BRAF Version 2.3.0 v2.3.0 criteria-combination framework: matched Rule15 (1 Pathogenic.Moderate + Pathogenic.Supporting >=4) with applied criteria: PS4 supporting, PM1 moderate, PM2 supporting, PM6 supporting, PP2 supporting, PP3 supporting, PP5 supporting; maps to Likely Pathogenic.
Classification rationale
PS4PM1PM2PM6PP2PP3PP5
Likely Pathogenic
BRAF c.736G>C
PS4 + PM1 + PM2 + PM6 + PP2 + PP3 + PP5
→
Likely Pathogenic
Gene diagram
· NM_001354609.1 · variants mapped to exon structure
BRAF
NM_001354609.1
Fetching transcript structure from UCSC…
Applied criteria · 7 applied · 12 assessed
Applied · 7
Strength
Supporting
Moderate
Strong
Very strong
✓
PS4
supporting
Pathogenic
This variant has been observed in multiple unrelated probands with cardio-facio-cutaneous (CFC) syndrome / RASopathy phenotype. It was identified among 8 BRAF mutations in 16 individuals from the original CFC cohort (Niihori et al. 2006). Nine independent clinical laboratories have submitted this variant as Pathogenic to ClinVar, and the ClinGen RASopathy VCEP has classified it as Pathogenic (VariationID 13965). The aggregate observation across multiple independent probands supports PS4 at a supporting level.
Reported in multiple CFC probands (Niihori 2006)ClinVar: 9 clinical labs + expert panel classification as PathogenicPMID:24409384 reports A246P as a CFC-causing mutant
✓
PM1
moderate
Pathogenic
The variant c.736G>C lies within exon 6 (c.712-860), which is one of the critical and well-established functional domains defined by the ClinGen RASopathy VCEP v2.3.0 (along with exon 11, P-loop AA 459-474, and CR3 activation segment AA 594-627). Exon 6 encodes part of the cysteine-rich domain (CRD) critical for BRAF function. The variant is absent from gnomAD, meeting the requirement of no benign variation in the domain.
c.736 is within exon 6 (CSPEC-defined critical domain)Variant absent from gnomAD v2.1 and v4.1
✓
PM2
supporting
Pathogenic
The variant is absent from gnomAD v2.1 and v4.1 population databases. Per the RASopathy VCEP v2.3.0, PM2 is applied at supporting strength when the variant is absent from gnomAD controls.
Absent from gnomAD v2.1 (exomes)Absent from gnomAD v4.1 (exomes/genomes)
✓
PM6
supporting
review
Pathogenic
Niihori et al. 2006 (PMID:16474404) reported a de novo occurrence of BRAF c.736G>C (p.Ala246Pro) in a proband with CFC syndrome where both parents tested negative for the variant. However, formal maternity/paternity confirmation was not performed, satisfying PM6 (assumed de novo without confirmed parentage) at supporting level (0.5 points) per the RASopathy VCEP point-based scoring system.
Niihori et al. 2006: de novo A246P in CFC probandparents negativeparentage not confirmed
✓
PP2
supporting
Pathogenic
BRAF has a high gnomAD missense z-score (well above 3.09), indicating strong constraint against missense variation in the general population. Missense variants are a common mechanism of disease for BRAF (gain-of-function in RASopathies). Per the RASopathy VCEP v2.3.0, PP2 is met at supporting strength when the gene's missense z-score exceeds 3.09 in gnomAD.
BRAF gnomAD missense z-score >3.09Missense variants are the predominant disease mechanism in BRAF-related RASopathies
✓
PP3
supporting
Pathogenic
The REVEL score for this missense variant is 0.928, which exceeds the threshold of ≥0.7 specified by the RASopathy VCEP v2.3.0 for PP3 at supporting strength. Multiple in silico tools support a deleterious effect on protein function.
REVEL score = 0.928 (≥0.7 threshold met)SpliceAI max delta = 0.05 (no significant splicing impact)
Assessed · not applied
Pathogenic
PS1
PS1 requires the same amino acid change to have been previously established as pathogenic through a different nucleotide change.
PS2
PS2 requires de novo occurrence with both maternity and paternity confirmed.
PS3
Functional evidence for this variant exists in the literature.
PM5
PM5 requires at least one different [likely] pathogenic residue change at the same codon (Ala246).
PP1
No cosegregation data were identified for this variant.
Benign
BA1
BA1 requires a gnomAD filtering allele frequency ≥0.05%.
BS1
BS1 requires a gnomAD filtering allele frequency ≥0.025% per the RASopathy VCEP v2.3.0.
BS2
BS2 requires observation of the variant in a healthy adult individual.
BS4
BS4 requires lack of segregation in affected family members.
BP2
BP2 requires observation of the variant in trans with a pathogenic variant in the same gene, or an alternative molecular cause of a RASopathy.
BP4
BP4 requires a REVEL score ≤0.3 for missense variants per the RASopathy VCEP v2.3.0.
BP5
BP5 requires an alternative molecular cause of a RASopathy in a different gene, with phenotype consistent with expected severity.
N/A · 9
PVS1 · PM3 · PM4 · PP4 · BS3 · BP1 · BP3 · BP6 · BP7
Research & evidence
Population frequency · supports pathogenic
gnomAD v4.1
gnomAD v2.1
v4.1
Absent from gnomAD v4.1.
v2.1
Absent from gnomAD v2.1.
🇨🇦 CA
This variant is absent from gnomAD-Canada.
Allele frequency by ancestry
three datasets · side by side
gnomAD v4.1
Absent
· 0 / ?
0 hom
0 hom
Not observed in any ancestry group.
gnomAD v2.1
Absent
· 0 / ?
0 hom
0 hom
Not observed in any ancestry group.
gnomAD Canada 🇨🇦
Absent
· 0 / ?
0 hom
0 hom
Not observed in any ancestry group.

ClinVar
This variant has been reported in ClinVar as Pathogenic (9 clinical laboratories) and as Pathogenic by ClinGen RASopathy Variant Curation Expert Panel (expert panel). (ClinVarID = 13965)
In silico
SpliceAI predicts no significant splice impact for this variant (max delta score = 0.05). REVEL score = 0.928. BayesDel score = 0.460772.
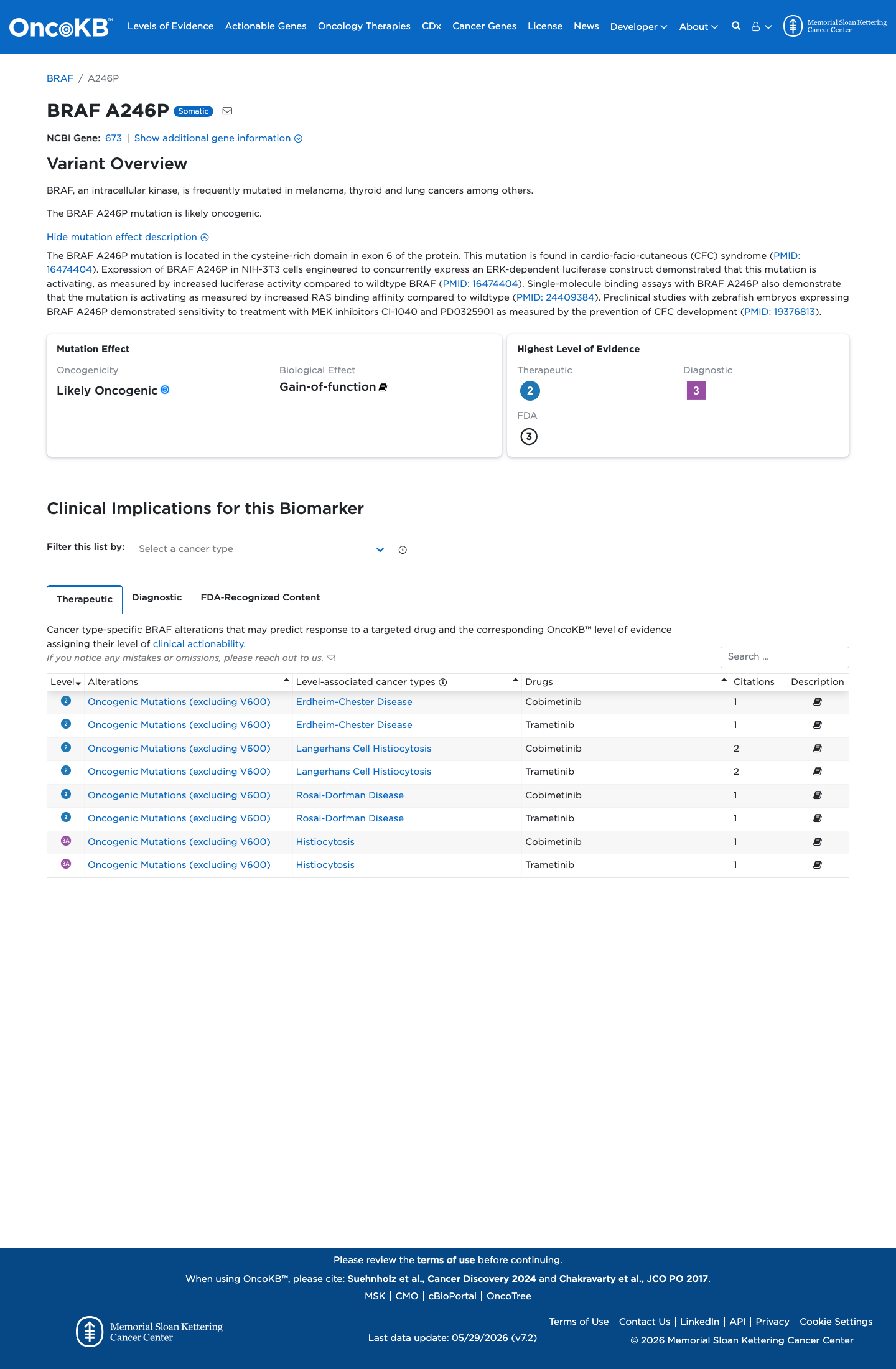
Functional
Likely Oncogenic
OncoKB identified variant-specific curated literature and context relevant to functional review; biological-effect context: Gain-of-function; curated oncogenicity label: Likely Oncogenic.

COSMIC
Cancer hotspots
Somatic evidence
Not in COSMIC / hotspots
COSMIC
This variant does not lie in a statistically significant hotspot. This variant has not previously been reported in somatic cancers (COSMIC).
Hotspots
This variant does not lie in a statistically significant hotspot.
Literature · how each cited paper was used
2papers cited
Each card is an audit: what was searched, what was found, whether it names the variant, which criteria it fed, and why. 6 further PMIDs triaged but not cited — see Sources & References.
Germline KRAS and BRAF mutations in cardio-facio-cutaneous syndrome.
Found
Structured finding pending for this record — see source link.
Applied to
→PM6 supports · met
→PS4 supports · met
Single-molecule force measurement via optical tweezers reveals different kinetic features of two BRaf mutants responsible for cardio-facial-cutaneous (CFC) syndrome.
Found
Reported in multiple CFC probands (Niihori 2006) ClinVar: 9 clinical labs + expert panel classification as Pathogenic PMID:24409384 reports A246P as a CFC-causing mutant
Applied to
→PS4 supports · met
Sources & reference links
Triaged references · 6 PMIDs not cited in assessment
19376813 ↗
Kinase-activating and kinase-impaired cardio-facio-cutaneous syndrome alleles have activity during zebrafish development and are sensitive to small molecule inhibitors.
ONCOKB
18042262 ↗
Mutation and phenotypic spectrum in patients with cardio-facio-cutaneous and Costello syndrome.
CLINVAR
24033266 ↗
A systematic approach to assessing the clinical significance of genetic variants.
CLINVAR
25741868 ↗
Standards and guidelines for the interpretation of sequence variants: a joint consensus recommendation of the American College of Medical Genetics and Genomics and the Association for Molecular Pathology.
CLINVAR
25173338 ↗
2014 ESC Guidelines on diagnosis and management of hypertrophic cardiomyopathy: the Task Force for the Diagnosis and Management of Hypertrophic Cardiomyopathy of the European Society of Cardiology (ESC).
CLINVAR
28492532 ↗
Sherloc: a comprehensive refinement of the ACMG-AMP variant classification criteria.
CLINVAR