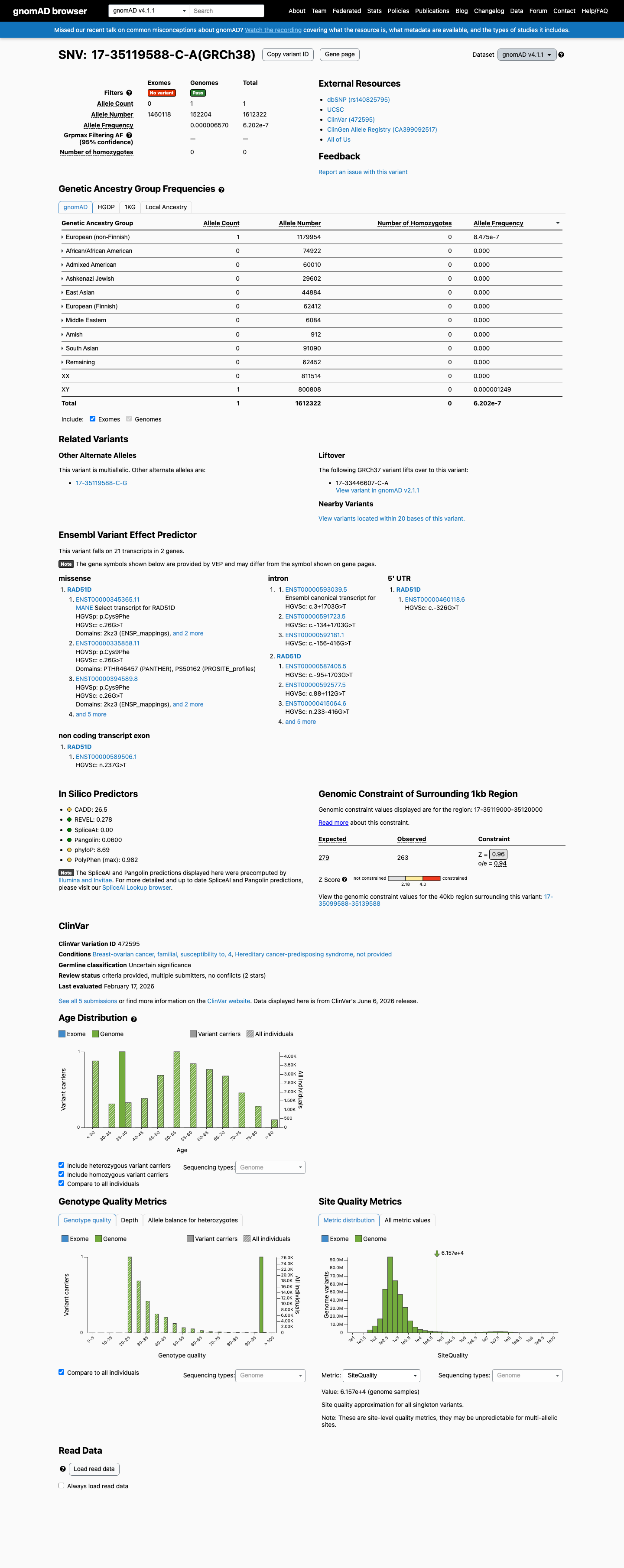
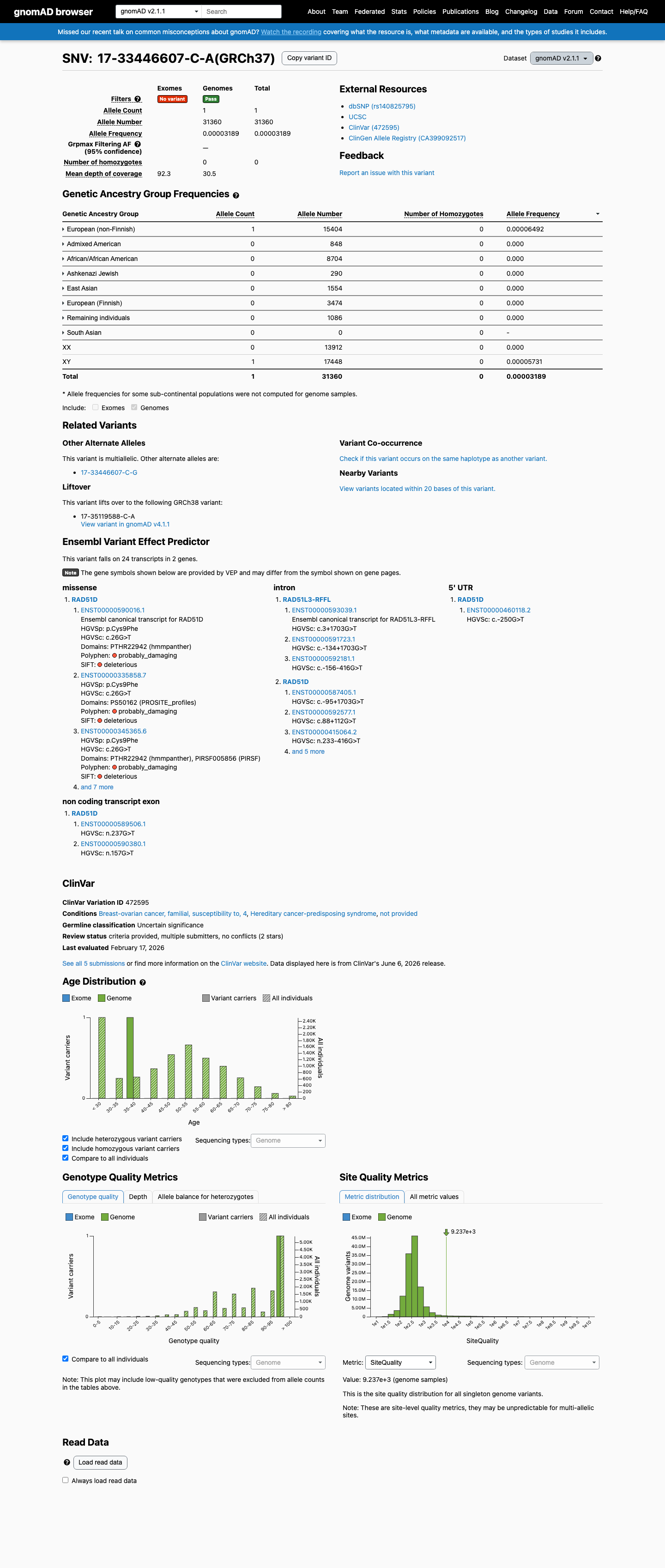
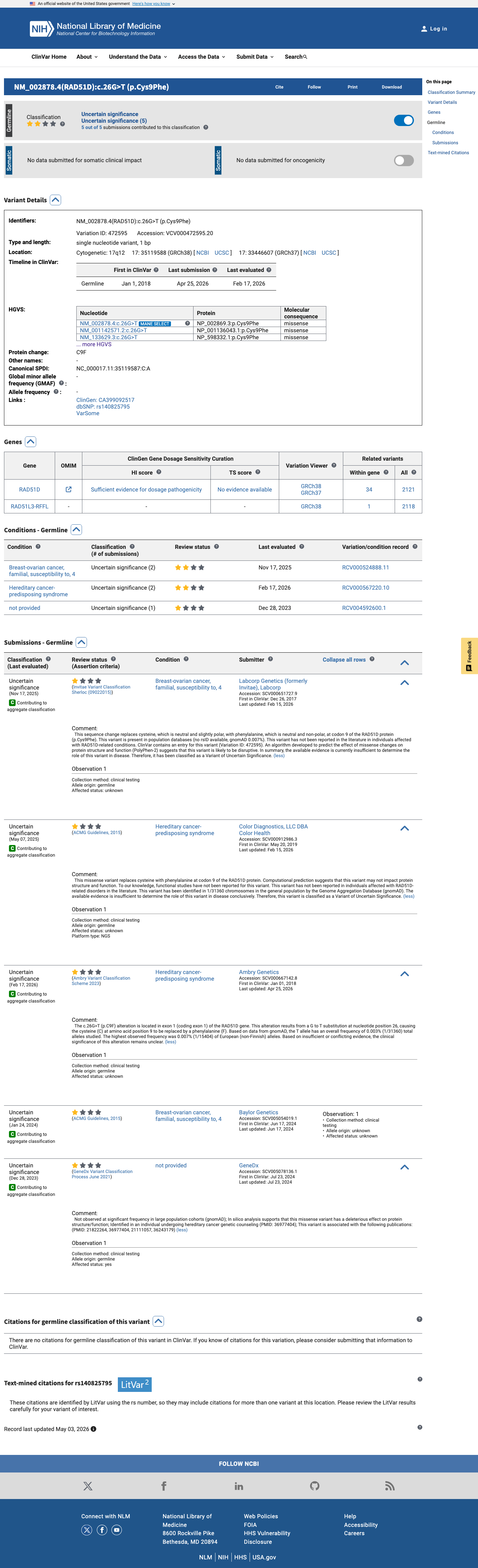
NM_002878.3:c.26G>T (p.Cys9Phe) is a missense variant in exon 1 of RAD51D, a gene associated with autosomal dominant hereditary breast and ovarian cancer predisposition. This variant is extremely rare in population databases: gnomAD v2.1 reports 1 allele in 31,360 (AF=0.00319%) and gnomAD v4.1 reports 1 allele in 1,612,322 (AF=0.00006%), meeting PM2 at supporting level.1 Multiple lines of computational evidence (REVEL 0.278, BayesDel 0.260, SpliceAI max delta 0.00) suggest this variant does not have a deleterious effect on protein function or splicing, meeting BP4 at supporting level.2 PVS1 is not applicable as this is a missense substitution, not a null variant.3 No functional studies, segregation data, de novo observations, case-control data, or pathogenic assertions from reputable sources are available for this variant.4 The variant has been reported in ClinVar as Uncertain significance by 5 clinical laboratories (ClinVar Variation ID: 472595), and has been observed once in somatic cancers (COSMIC COSV50100981).5 The net evidence profile (PM2_supporting + BP4_supporting) results in an overall classification of Uncertain significance under ACMG/AMP 2015 combination rules.
RAD51D
Final classification
VUS
RAD51D c.26G>T · p.Cys9Phe
RAD51D
NM_002878.3:c.26G>T (p.Cys9Phe) is a missense variant in exon 1 of RAD51D, a gene associated with autosomal dominant hereditary breast and ovarian cancer predisposition.
gene-specific framework lacked a usable explicit final combination framework, so generic ACMG/AMP 2015 final-combination rules were applied as fallback; applied criteria: PM2 supporting, BP4 supporting; combination = 1 supporting + 1 supporting benign, which maps to VUS.
Classification rationale
PM2
BP4
VUS
RAD51D c.26G>T
PM2 + BP4
→
VUS
2
revelbayesdelspliceai ↗
3
pvs1_gene_contextpvs1_variant_assessment
Gene diagram
· NM_002878.3 · variants mapped to exon structure
RAD51D
NM_002878.3
Fetching transcript structure from UCSC…
Applied criteria · 2 applied · 21 assessed
Applied · 2
Strength
Supporting
Moderate
Strong
Very strong
✓
PM2
supporting
Pathogenic
This variant is extremely rare in population databases. gnomAD v2.1 reports 1 allele in 31,360 (AF=0.00319%), and gnomAD v4.1 reports 1 allele in 1,612,322 (AF=0.00006%). Both frequencies are well below the 0.1% threshold for PM2. The variant is absent from gnomAD-Canada.
gnomAD v2.1: AF=0.00319% (1/31360)homozygous=0
✓
BP4
supporting
Benign
Multiple lines of computational evidence suggest this variant does not impact protein function or splicing. REVEL score of 0.278 is well below the pathogenic threshold of 0.5. BayesDel score of 0.260 is weakly positive. SpliceAI predicts no splicing impact (max delta = 0.00). The weight of in silico evidence supports a benign interpretation.
REVEL: 0.278 — below pathogenic threshold of 0.5BayesDel: 0.260 — low positive scoreSpliceAI: max delta = 0.00 — no predicted splicing alteration
Assessed · not applied
Pathogenic
PVS1
NM_002878.3:c.26G>T is a missense variant (p.Cys9Phe) in exon 1 and does not fall into any PVS1 null-variant category (nonsense, frameshift, or canonical ±1,2 splice consensus).
PS1
No alternate nucleotide change at position c.26 has been reported as pathogenic in ClinVar or the literature.
PS2
No de novo observations have been reported for this variant.
PS3
No variant-specific functional studies have been reported.
PS4
No case-control studies demonstrate statistically significant enrichment of this variant in affected individuals versus controls.
PM1
The variant does not lie within a statistically significant mutational hotspot.
PM6
No de novo observations have been reported for this variant.
PP1
No segregation data are available for this variant.
PP2
Insufficient gene-level data to determine whether RAD51D has a low rate of benign missense variation and whether missense variants are a common mechanism of disease.
PP3
Multiple in silico predictors do not support a deleterious effect.
PP4
No specific phenotype or family history data are available for individuals carrying this variant.
PP5
No reputable source has classified this variant as pathogenic.
Benign
BA1
The maximum allele frequency observed in any population is 0.00649% (gnomAD v2.1, European non-Finnish).
BS1
The maximum allele frequency observed is 0.00649% (gnomAD v2.1 NFE), well below the 0.3% threshold for BS1.
BS2
The variant has not been observed in a homozygous state in gnomAD (0 homozygotes in both v2.1 and v4.1), and no data exist demonstrating observation in healthy adult controls without disease.
BS3
No variant-specific functional studies demonstrating a neutral or benign effect have been reported.
BS4
No evidence is available demonstrating lack of segregation with disease in affected families.
BP1
RAD51D is a gene in which both missense and truncating variants can be pathogenic.
BP2
No observation of this variant in trans with a known pathogenic RAD51D variant has been reported for a fully penetrant dominant disorder.
BP5
No alternative molecular basis for disease has been identified in individuals carrying this variant.
BP6
No reputable source classifies this variant as benign.
N/A · 5
PM3 · PM4 · PM5 · BP3 · BP7
Research & evidence
Population frequency
gnomAD v4.1
gnomAD v2.1
v4.1
This variant is present in gnomAD v4.1 (AF= 6.20224e-07; MAF= 0.00006%, 1/1612322 alleles, homozygotes = 0) and has highest observed frequency in the European (non-Finnish) population (AF= 8.47491e-07; MAF= 0.00008%, 1/1179954 alleles, homozygotes = 0).
v2.1
This variant is present in gnomAD v2.1 (AF= 3.18878e-05; MAF= 0.00319%, 1/31360 alleles, homozygotes = 0) and has highest observed frequency in the European (non-Finnish) population (AF= 6.49182e-05; MAF= 0.00649%, 1/15404 alleles, homozygotes = 0).
🇨🇦 CA
Absent from gnomAD-Canada v1.0.
Allele frequency by ancestry
three datasets · side by side
gnomAD v4.1
6.2e-05%
· 1 / 1,612,322
0 hom
0 hom
European (non-Finnish) 1 / 1,179,954 |
8.5e-05% |
+ 9 not observed (Remaining individuals, Admixed American, European (Finnish), Amish, East Asian, Middle Eastern, South Asian, Ashkenazi Jewish, African/African American)
gnomAD v2.1
0.0032%
· 1 / 31,360
0 hom
0 hom
European (non-Finnish) 1 / 15,404 |
0.0065% |
+ 7 not observed (African/African American, Admixed American, Ashkenazi Jewish, East Asian, European (Finnish), Remaining individuals, South Asian)
gnomAD Canada 🇨🇦
Absent
· 0 / ?
0 hom
0 hom
Not observed in any ancestry group.
ClinVar
This variant has been reported in ClinVar as Uncertain significance (5 clinical laboratories). (ClinVarID = 472595)
In silico
SpliceAI predicts no significant splice impact for this variant (max delta score = 0.00). REVEL score = 0.278. BayesDel score = 0.260344.
Functional
Unknown Oncogenic Effect
OncoKB did not identify variant-specific reviewed functional evidence for this variant; gene-level curated context is available for reviewer follow-up. RAD51D, a DNA repair protein, is infrequently altered in cancer.
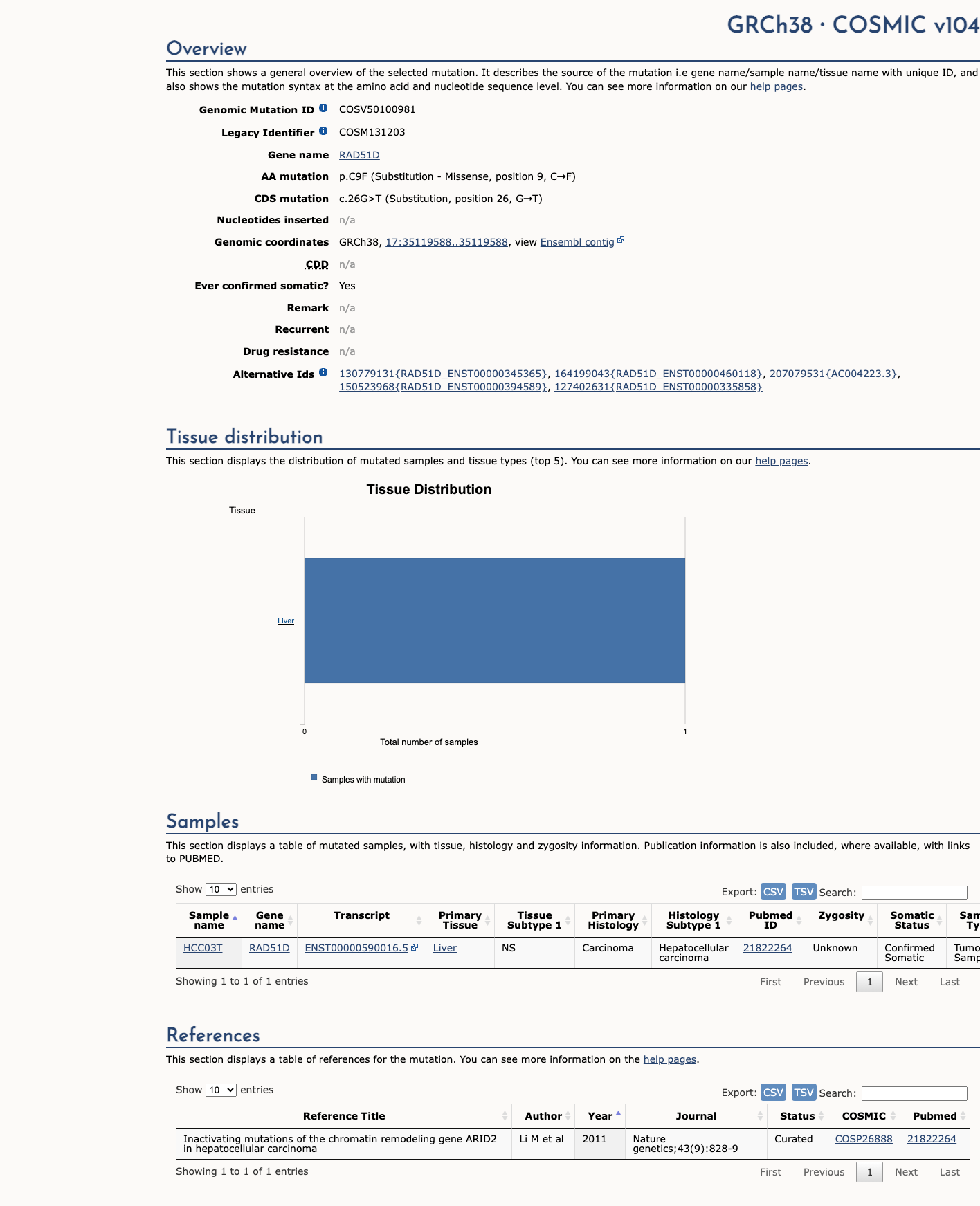
COSMIC
Cancer hotspots
Somatic evidence
Not in COSMIC / hotspots
COSMIC
This variant does not lie in a statistically significant hotspot. This variant has previously been reported in somatic cancers (COSMIC; COSV50100981, n = 1 times).
Hotspots
This variant does not lie in a statistically significant hotspot.
Sources & reference links
Triaged references · 2 PMIDs not cited in assessment
25741868 ↗
Standards and guidelines for the interpretation of sequence variants: a joint consensus recommendation of the American College of Medical Genetics and Genomics and the Association for Molecular Pathology.
CLINVAR
25394175 ↗
A practice guideline from the American College of Medical Genetics and Genomics and the National Society of Genetic Counselors: referral indications for cancer predisposition assessment.
CLINVAR